

Patterns of chemotherapy-associated toxicity and supportive care in US oncology practice: a nationwide prospective cohort study
- PMID: 24706592
- PMCID: PMC3987093
- DOI: 10.1002/cam4.200
Patterns of chemotherapy-associated toxicity and supportive care in US oncology practice: a nationwide prospective cohort study
Abstract
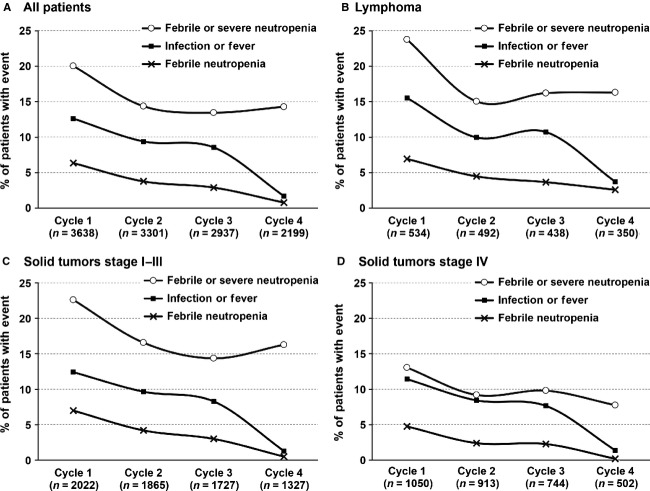
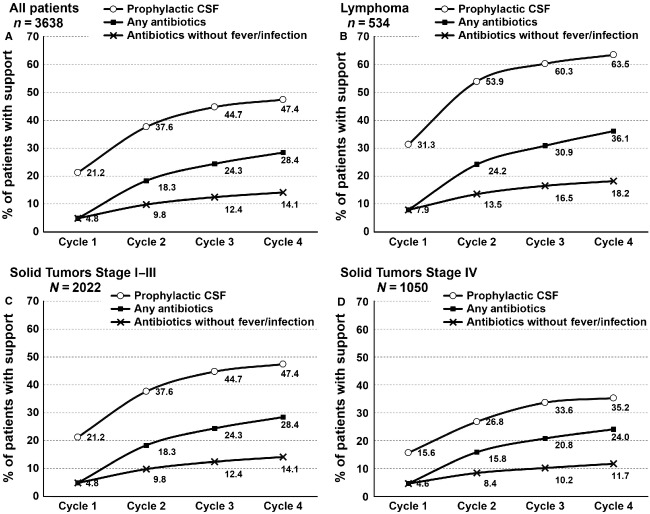
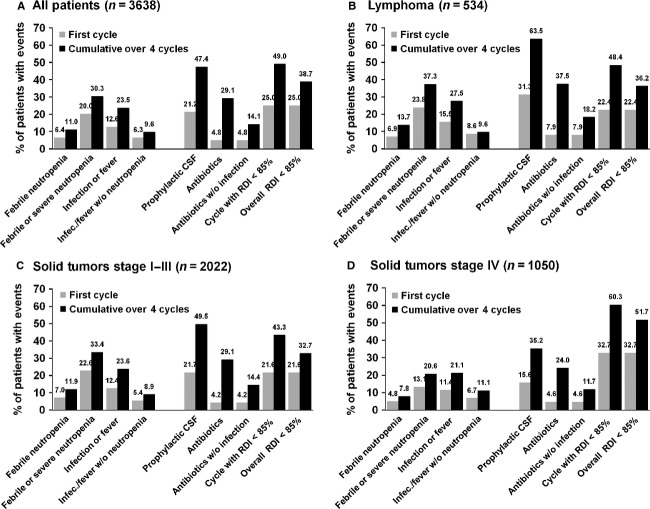
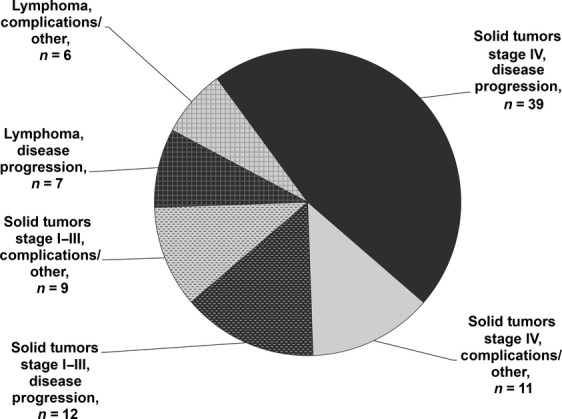
Neutropenic complications remain an important dose-limiting toxicity of cancer chemotherapy-associated with considerable morbidity, mortality, and cost. Risk of the initial neutropenic event is greatest during the first cycle. The purpose of this study was to better understand timing of neutropenic events in relation to delivered chemotherapy dose intensity and utilization of supportive care during cancer treatment. A prospective cohort study of adult patients with solid tumors or lymphoma initiating chemotherapy was conducted at 115 randomly selected US practice sites between 2002 and 2006. Chemotherapy-associated toxicities were captured in up to four treatment cycles including severe neutropenia, febrile neutropenia, and infection. Documented interventions included colony-stimulating factor (CSF), antibiotics use, and reductions in chemotherapy relative dose intensity (RDI). A total of 3638 patients with breast (39.7%), lung (23.7%), colorectal (13.6%), ovarian (8.3%) cancers, or lymphoma (14.7%) were eligible for this analysis. The majority of neutropenic and infection events occurred in the first cycle. A significant inverse relationship was observed between reductions in neutropenic and infectious events and increased utilization of measures to reduce these complications in subsequent cycles. More than 60% of patients with stage IV solid tumors underwent reductions in RDI. Patients with lymphoma and stage I-III solid tumors had less dose reductions while receiving more prophylactic CSFs. Approximately, 15% of patients received prophylactic antibiotics. While the risk of neutropenic complications remains greatest during the initial cycle of chemotherapy, subsequently instituted clinical measures in efforts to reduce the risk of these events vary with cancer type and stage.
Keywords: Chemotherapy; infection; neutropenia; toxicity.
© 2014 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Figures
References
-
- Kuderer NM, Dale DC, Crawford J, Cosler LE, Lyman GH. Mortality, morbidity, and cost associated with febrile neutropenia in adult cancer patients. Cancer. 2006;106:2258–2266. - PubMed
-
- Lewis MA, Hendrickson AW, Moynihan TJ. Oncologic emergencies: pathophysiology, presentation, diagnosis, and treatment. CA Cancer J. Clin. 2011;61:287–314. - PubMed
-
- Klastersky JA, Paesmans M. Treatment of febrile neutropenia is expensive: prevention is the answer. Onkologie. 2011;34:226–228. - PubMed
-
- Liou SY, Stephens JM, Carpiuc KT, Feng W, Botteman MF, Hay JW. Economic burden of haematological adverse effects in cancer patients: a systematic review. Clin. Drug Investig. 2007;27:381–396. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
