

A randomized trial of real-time automated clinical deterioration alerts sent to a rapid response team
- PMID: 24706596
- PMCID: PMC4354800
- DOI: 10.1002/jhm.2193
A randomized trial of real-time automated clinical deterioration alerts sent to a rapid response team
Abstract
Background: Episodes of patient deterioration on hospital units are expected to increasingly contribute to morbidity and healthcare costs.
Objective: To determine if real-time alerts sent to the rapid response team (RRT) improved patient care.
Design: Randomized, controlled trial.
Setting: Eight medicine units (Barnes-Jewish Hospital).
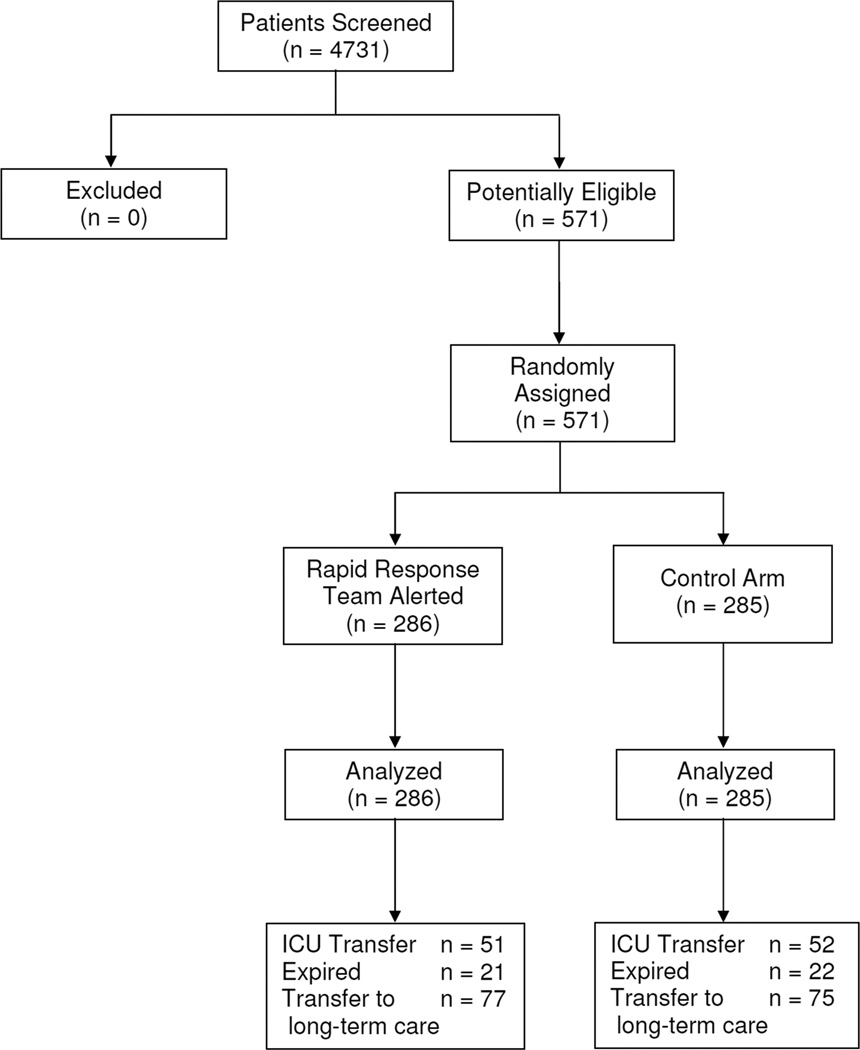
Patients: Five hundred seventy-one patients.
Intervention: Real-time alerts generated by a validated deterioration algorithm were sent real-time to the RRT (intervention) or hidden (control).
Measurements: Intensive care unit (ICU) transfer, hospital mortality, hospital duration.
Results: ICU transfer (17.8% vs 18.2%; odds ratio: 0.972; 95% confidence interval [CI]: 0.635-1.490) and hospital mortality (7.3% vs 7.7%; odds ratio: 0.947; 95% CI: 0.509-1.764) were similar for the intervention and control groups. The number of patients requiring transfer to a nursing home or long-term acute care hospital was similar for patients in the intervention and control groups (26.9% vs 26.3%; odds ratio: 1.032; 95% CI: 0.712-1.495). Hospital duration (8.4 ± 9.5 days vs 9.4 ± 11.1 days; P = 0.038) was statistically shorter for the intervention group. The number of RRT calls initiated by the primary care team was similar for the intervention and control groups (19.9% vs 16.5%; odds ratio: 1.260; 95% CI: 0.823-1.931).
Conclusions: Real-time alerts sent to the RRT did not reduce ICU transfers, hospital mortality, or the need for subsequent long term care. However, hospital length of stay was modestly reduced.
© 2014 Society of Hospital Medicine.
Conflict of interest statement
References
-
- Hillman KM, Bristow PJ, Chey T, et al. Duration of life-threatening antecedents prior to intensive care admission. Intensive Care Med. 2002;28(11):1629–1634. - PubMed
-
- Kause J, Smith G, Prytherch D, et al. A comparison of antecedents to cardiac arrests, deaths and emergency intensive care admissions in Australia and New Zealand, and the United Kingdom--the ACADEMIA study. Resuscitation. 2004;62(3):275–282. - PubMed
-
- Lighthall GK, Markar S, Hsiung R. Abnormal vital signs are associated with an increased risk for critical events in US veteran inpatients. Resuscitation. 2009;80(11):1264–1269. - PubMed
-
- Lundberg JS, Perl TM, Wiblin T, et al. Septic shock: an analysis of outcomes for patients with onset on hospital wards versus intensive care units. Crit Care Med. 1998;26(6):1020–1024. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
