

Gastric adenocarcinoma presenting with gastric outlet obstruction in a child
- PMID: 24707411
- PMCID: PMC3965945
- DOI: 10.1155/2014/527471
Gastric adenocarcinoma presenting with gastric outlet obstruction in a child
Abstract
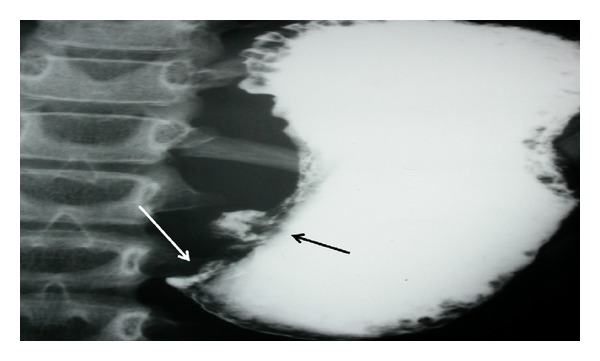
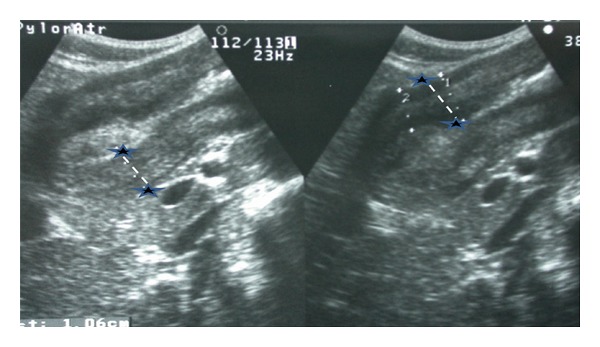
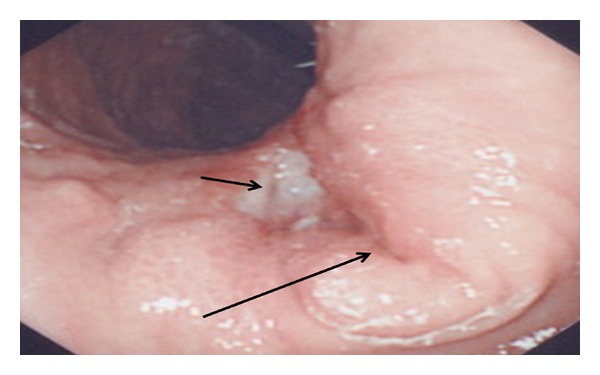
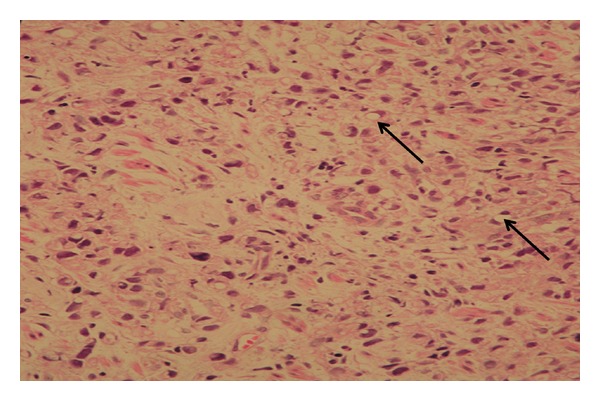
Gastric carcinoma is extremely rare in children representing only 0.05% of all gastrointestinal malignancies. Here, we report the first pediatric case of gastric cancer presenting with gastric outlet obstruction. Upper endoscopy revealed a markedly thickened antral mucosa occluding the pylorus and a clean base ulcer 1.5 cm × 2 cm at the lesser curvature of the stomach. The narrowed antrum and pylorus underwent balloon dilation, and biopsy from the antrum showed evidence of Helicobacter pylori gastritis. The biopsy taken from the edge of the gastric ulcer demonstrated signet-ring-cell type infiltrate consistent with gastric adenocarcinoma. At laparotomy, there were metastases to the liver, head of pancreas, and mesenteric lymph nodes. Therefore, the gastric carcinoma was deemed unresectable. The patient died few months after initiation of chemotherapy due to advanced malignancy. In conclusion, this case report underscores the possibility of gastric adenocarcinoma occurring in children and presenting with gastric outlet obstruction.
Figures
References
-
- Brecht IB, Graf N, Schweinitz DV, Frühwald MC, Bielack SS, Schneider DT. Networking for children and adolescents with very rare tumors: foundation of the gpoh pediatric rare tumor group. Klinische Padiatrie. 2009;221(3):181–185. - PubMed
-
- Goldthorn JF, Canizaro PC. Gastrointestinal malignancies in infancy, childhood, and adolescence. Surgical Clinics of North America. 1986;66(4):845–861. - PubMed
-
- International Agency for Research on Cancer (IARC) Globocan 2002, http://globocan.iarc.fr/
-
- Oncology Center at King Faisal Specialist Hospital and Research Center in Riyadh-Saudi Arabia. The 2010 tumor registry annual report. http://www.kfshrc.edu.sa/KFCCC/AnnualReports/2010%20Tumor%20Registry%20A....
-
- Harting MT, Blakely ML, Herzog CE, Lally KP, Ajani JA, Andrassy RJ. Treatment issues in pediatric gastric adenocarcinoma. Journal of Pediatric Surgery. 2004;39(8):e8–e10. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
