

Analysis of enamel surface damage after selective laser ablation of composite from tooth surfaces
- PMID: 24707453
- PMCID: PMC3972898
- DOI: 10.1515/plm-2013-0052
Analysis of enamel surface damage after selective laser ablation of composite from tooth surfaces
Abstract
Objective: Resin-based composites are used for many applications in dentistry. They are difficult to remove without damage to the underlying enamel since they adhere strongly and are color matched to the tooth. The objective of this study was to determine if an automated laser scanning system with spectral feedback could be used for selective removal of residual orthodontic composite from tooth surfaces with minimal damage to the underlying enamel.
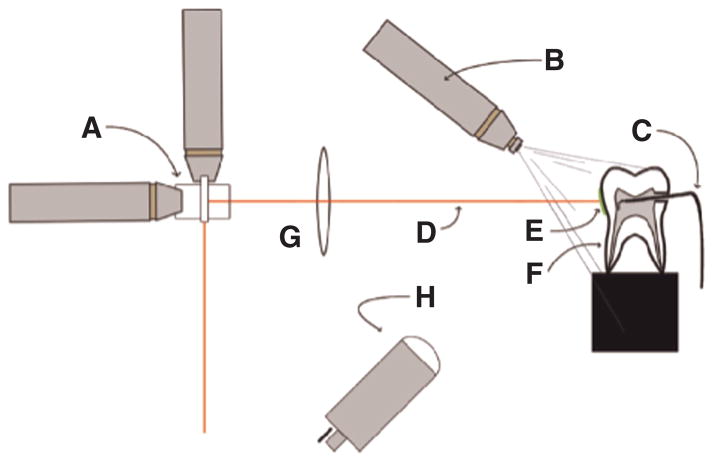
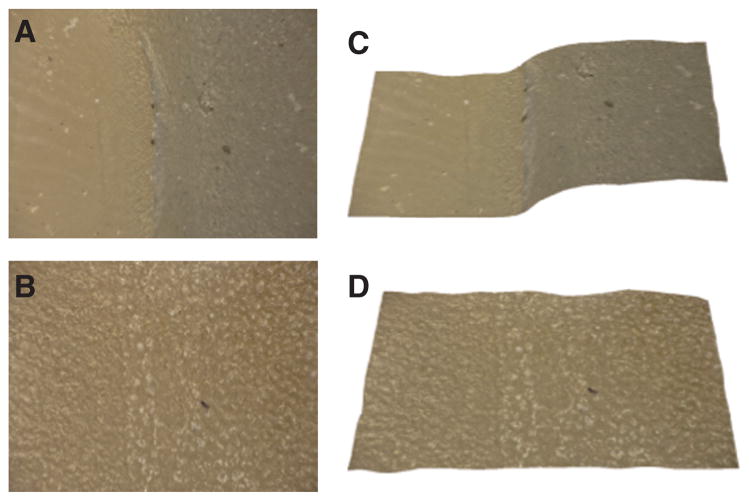
Materials and methods: A CO2 laser operating at a wavelength of 9.3 μm with a pulse duration of 10-15 μs and a pulse repetition rate of ~200 Hz was used to selectively remove composite from the buccal surfaces of extracted teeth. A spectral feedback system utilizing a miniature spectrometer was used to control the laser scanning system. Pulpal temperature measurements were performed during composite removal to determine if there was excessive heat accumulation. Conventional and digital microscopes were used to assess the amount of enamel lost during removal.
Results: The amount of enamel lost averaged between 20 and 25 μm for irradiation intensities from 3.8 to 4.2 J/cm2, respectively. An average maximum temperature rise of 1.9±1.5°C was recorded, with no teeth approaching the critical value of 5.5°C. The average time for composite removal from an area of 5 mm2 was 19.3±4.1 s, fast enough for clinical feasibility.
Conclusion: Residual composite can be rapidly removed from tooth surfaces using a CO2 laser with spectral feedback, with minimal temperature rise within the pulp and with minimal loss of sound enamel.
Keywords: carbon dioxide laser; composite removal; laser ablation.
Conflict of interest statement
Figures





References
-
- Bernardo M, Luis H, Martin MD, Leroux BG, Rue T, Leitão J, DeRouen TA. Survival and reasons for failure of amalgam versus composite posterior restorations placed in a randomized clinical trial. J Am Dent Assoc. 2007;138(6):775–83. - PubMed
-
- Oliver RG. The effect of different methods of bracket removal on the amount of residual adhesive. Am J Orthod Dentofacial Orthop. 1988;93(3):196–200. - PubMed
-
- Hong YH, Lew KK. Quantitative and qualitative assessment of enamel surface following five composite removal methods after bracket debonding. Eur J Orthod. 1995;17(2):121–8. - PubMed
-
- Ryf S, Flury S, Palaniappan S, Lussi A, van Meerbeek B, Zimmerli B. Enamel loss and adhesive remnants following bracket removal and various clean-up procedures in vitro. Eur J Orthod. 2012;34(1):25–32. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources