

Hashimoto's thyroiditis pathology and risk for thyroid cancer
- PMID: 24708347
- PMCID: PMC4080848
- DOI: 10.1089/thy.2013.0588
Hashimoto's thyroiditis pathology and risk for thyroid cancer
Abstract
Background: Hashimoto's thyroiditis (HT) has been found to coexist with differentiated thyroid cancer (DTC) in surgical specimens, but an association between the two conditions has been discounted by the medical literature. Therefore, we performed this study to determine any potential relationship between HT and the risk of developing DTC.
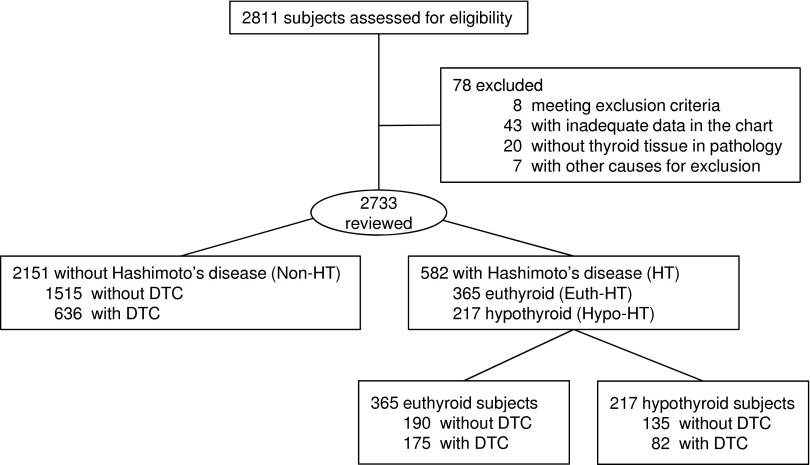
Methods: We collected data for thyrotropin (TSH), thyroxine (T4), thyroid peroxidase antibody (TPO-Ab) titers, surgical pathology, and weight-based levothyroxine (LT4) replacement dose for patients who were referred for thyroid surgery. Patients with HT at final pathology were studied further. To estimate thyroid function, patients with preoperative hypothyroid HT (Hypo-HT) were divided into three equal groups based on their LT4 replacement: LT4-Low (<0.90 μg/kg), LT4-Mid (0.90-1.43 μg/kg), and LT4-High (>1.43 μg/kg). A group of preoperatively euthyroid (Euth-HT) patients but with HT by pathology was also studied. All subjects were also grouped based on their TPO-Ab titer in TPO-high (titer >1:1000) or TPO-low/negative (titer <1:1000 or undetectable) groups. The relationship of HT and DTC was studied extensively.
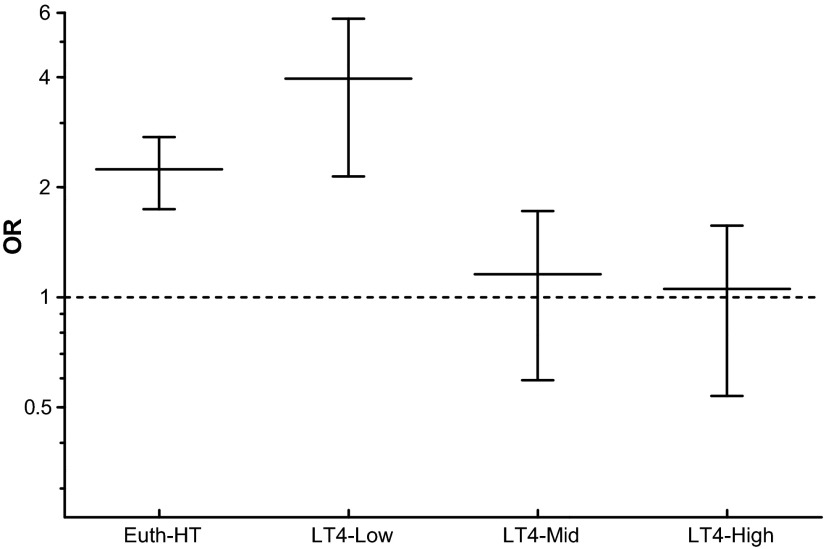
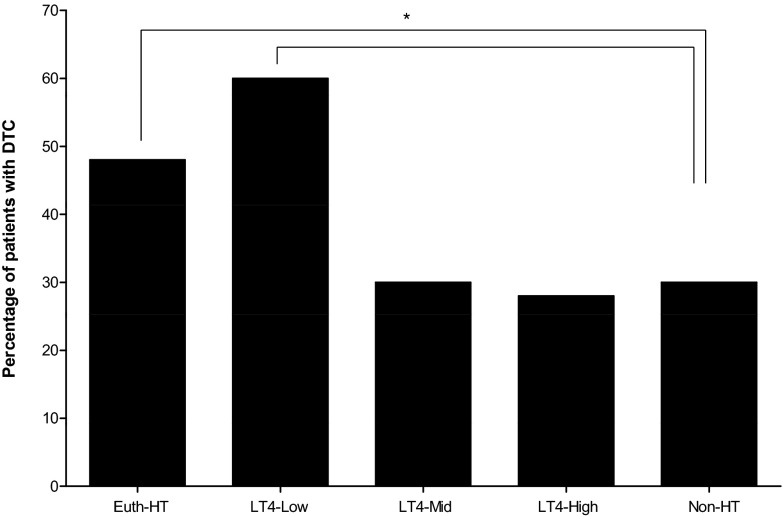
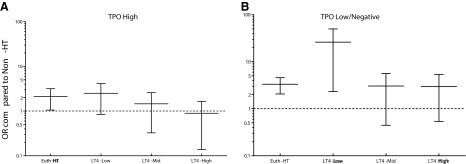
Results: Of 2811 subjects, 582 had HT on surgical pathology, 365 of whom were Euth-HT preoperatively. DTC was present in 47.9% of the Euth-HT, in 59.7% of LT4-Low, 29.8% of LT4-Mid, and 27.9% of LT4-High groups. The relative risk (RR) for DTC was significantly elevated for the Euth-HT and LT4-Low groups (p<0.001), but not for the LT4-Mid or LT4-High replacement dose groups. TPO-low/negative status conferred an increased RR in the Euth-HT and LT4-Low replacement dose groups (p<0.001 both), while TPO-high status decreased it in Euth-HT group (p<0.05) and made it nonsignificant in the LT4-Low group.
Conclusions: HT pathology increases the risk for DTC only in euthyroid subjects and those with partially functional thyroid glands (LT4-Low) but not in fully hypothyroid HT (LT4-Mid and LT4-High). High TPO-Ab titers appear to protect against DTC in patients with HT.
Figures
Comment in
-
Thyroid gland. Unlocking the potential of thyroid autoantibodies.Nat Rev Endocrinol. 2014 Jun;10(6):314. doi: 10.1038/nrendo.2014.63. Epub 2014 Apr 29. Nat Rev Endocrinol. 2014. PMID: 24776731 No abstract available.
-
Oh, no--equations! Reanalysis of the data reveal even stronger associations between Hashimoto's thyroiditis and differentiated thyroid cancer.Thyroid. 2015 Jan;25(1):141-2. doi: 10.1089/thy.2014.0301. Thyroid. 2015. PMID: 25072275 No abstract available.
-
Response to: "Oh, no--equations! Reanalysis of the data reveal even stronger associations between Hashimoto's thyroiditis and differentiated thyroid cancer".Thyroid. 2015 Jan;25(1):142. doi: 10.1089/thy.2014.0493. Thyroid. 2015. PMID: 25375759 No abstract available.
References
-
- Li N, Du XL, Reitzel LR, Xu L, Sturgis EM.2013Impact of enhanced detection on the increase in thyroid cancer incidence in the United States: review of incidence trends by socioeconomic status within the Surveillance, Epidemiology, and End Results registry, 1980–2008. Thyroid 23:103–110 - PMC - PubMed
-
- Chen H, Schneider D, Mazeh H, Jaume JC, Lubner S.2013Endocrine Cancer. In: Abeloff MD, Armitage JO, Niederhuber JE, Kastan MB, McKenna WG. (eds) Abeloff's Clinical Oncology, 5th edition. Churchill Livingstone Elsevier, Philadelphia, PA, pp. 1112–1142
-
- Braverman LE.1994Iodine and the thyroid: 33 years of study. Thyroid 4:351–356 - PubMed
-
- Virchow R.1956Standpoints in Scientific Medicine, 1877. Bull Hist Med 30:537–543 - PubMed
-
- Balkwill F, Mantovani A.2001Inflammation and cancer: back to Virchow? Lancet 357:539–545 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
