

Increased respiratory drive relates to severity of dyspnea in systemic sclerosis
- PMID: 24708492
- PMCID: PMC3986445
- DOI: 10.1186/1471-2466-14-57
Increased respiratory drive relates to severity of dyspnea in systemic sclerosis
Abstract
Background: Dyspnea may be a presenting symptom in progressive systemic sclerosis (SSc). Respiratory drive (mouth occlusion pressure, MOP, at rest and during CO2 rebreathing, 7% CO2, 93% O2) is a major determinant of dyspnea and may relate to the magnitude of dyspnea.
Methods: In a prospective design, MOP at 0.1 sec (P0.1) was measured in 73 SSc patients while breathing room air and during CO2 rebreathing. An abnormal V'E/P0.1 is defined as < 8 L/min/cm H2O. Dyspnea scores were assessed by a shortness of breath questionnaire (UCSD dyspnea scale).
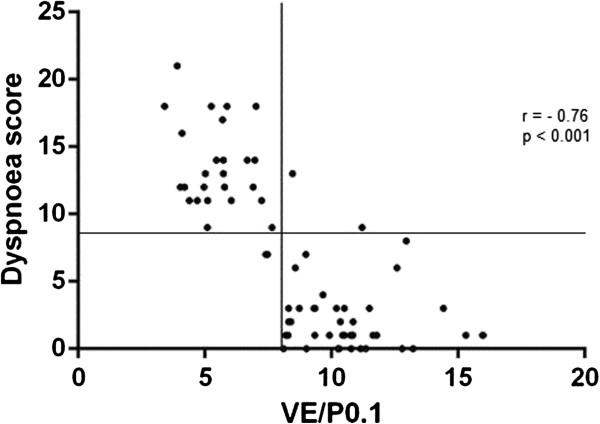
Results: Mean P0.1 in patients with normal V'E/P0.1 (n = 45) was 1.1 ± 0.04 and 1.6 ± 0.08 cm H2O in patients with abnormal V'E/P0.1 (n = 28), p <0.001. ∆P0.1/∆PetCO2 differed significantly between these groups (0.45 versus 0.75 cm H2O/mmHg, P < 0.001), but no significant difference was present in ∆V'E/∆PetCO2. V'E/P0.1 showed the highest significant correlation with the UCSD dyspnea score (r = -0.76, p <0.001). UCSD cut-off value for abnormal V'E/P0.1 was 8.5 (sensitivity 93%, specificity 96%, area under the curve 0.98).
Conclusions: In SSc patients an abnormal V'E/P0.1 better relates to the severity of dyspnea than traditional lung function parameters and can easily be assessed at first outpatient consultation.
Figures
Similar articles
-
The global peripheral chemoreflex drive in patients with systemic sclerosis: a rebreathing and exercise study.QJM. 2015 Jan;108(1):33-8. doi: 10.1093/qjmed/hcu150. Epub 2014 Jul 13. QJM. 2015. PMID: 25024353
-
Minute ventilation/carbon dioxide production in chronic heart failure.Eur Respir Rev. 2021 Feb 2;30(159):200141. doi: 10.1183/16000617.0141-2020. Print 2021 Mar 31. Eur Respir Rev. 2021. PMID: 33536259 Free PMC article.
-
Minute ventilation to carbon dioxide output (V'E/V'CO2 slope) is the strongest death predictor before larger lung resections.Monaldi Arch Chest Dis. 2017 Sep 22;87(3):817. doi: 10.4081/monaldi.2017.817. Monaldi Arch Chest Dis. 2017. PMID: 29424191
-
Ventilatory response to exercise in cardiopulmonary disease: the role of chemosensitivity and dead space.Eur Respir J. 2018 Feb 7;51(2):1700860. doi: 10.1183/13993003.00860-2017. Print 2018 Feb. Eur Respir J. 2018. PMID: 29437936 Review.
-
Physiological and clinical relevance of exercise ventilatory efficiency in COPD.Eur Respir J. 2017 Mar 8;49(3):1602036. doi: 10.1183/13993003.02036-2016. Print 2017 Mar. Eur Respir J. 2017. PMID: 28275174 Review.
Cited by
-
Respiratory Drive and Survival in Comatose Out-of-Hospital Post-Cardiac Arrest Patients.Open Access Emerg Med. 2025 Aug 21;17:233-245. doi: 10.2147/OAEM.S511715. eCollection 2025. Open Access Emerg Med. 2025. PMID: 40860239 Free PMC article.
References
-
- Black CM, Stephen C. In: Oxford Textbook of Rheumatology. MadisonPJ IDA, WooP GDN, editor. Oxford: Oxford University Press; 1993. Systemic Sclerosis (Scleroderma) And Related Disorders; p. 771.
-
- LeRoy EC, Black C, Fleischmajer R, Jablonska S, Krieg T, Medsger TA Jr, Rowell N, Wollheim F. Scleroderma (systemic sclerosis): classification, subsets and pathogenenis. J Rheumatol. 1988;15:202–205. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
