

Birth Preparedness and Complication Readiness (BPCR) interventions to reduce maternal and neonatal mortality in developing countries: systematic review and meta-analysis
- PMID: 24708719
- PMCID: PMC4234142
- DOI: 10.1186/1471-2393-14-129
Birth Preparedness and Complication Readiness (BPCR) interventions to reduce maternal and neonatal mortality in developing countries: systematic review and meta-analysis
Abstract
Background: Birth Preparedness and Complication Readiness (BPCR) interventions are widely promoted by governments and international agencies to reduce maternal and neonatal health risks in developing countries; however, their overall impact is uncertain, and little is known about how best to implement BPCR at a community level. Our primary aim was to evaluate the impact of BPCR interventions involving women, families and communities during the prenatal, postnatal and neonatal periods to reduce maternal and neonatal mortality in developing countries. We also examined intervention impact on a variety of intermediate outcomes important for maternal and child survival.
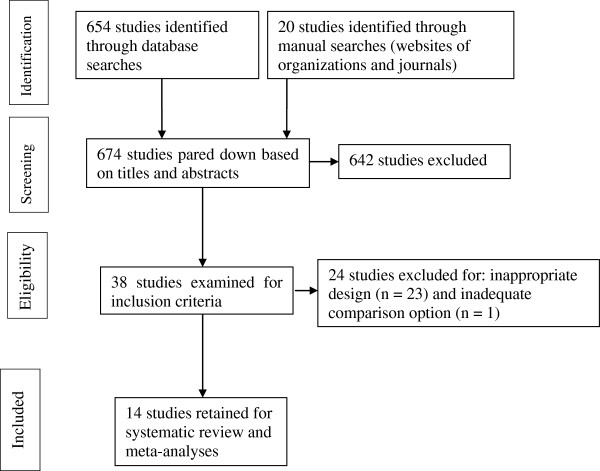
Methods: We conducted a systematic review and meta-analysis of randomized trials of BPCR interventions in populations of pregnant women living in developing countries. To identify relevant studies, we searched the scientific literature in the Pubmed, Embase, Cochrane library, Reproductive health library, CINAHL and Popline databases. We also undertook manual searches of article bibliographies and web sites. Study inclusion was based on pre-specified criteria. We synthesised data by computing pooled relative risks (RR) using the Cochrane RevMan software.
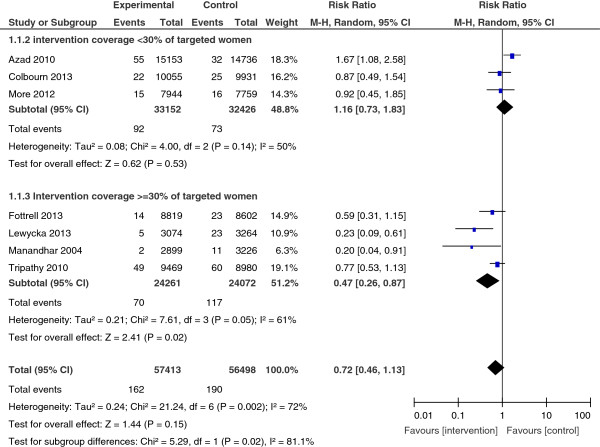
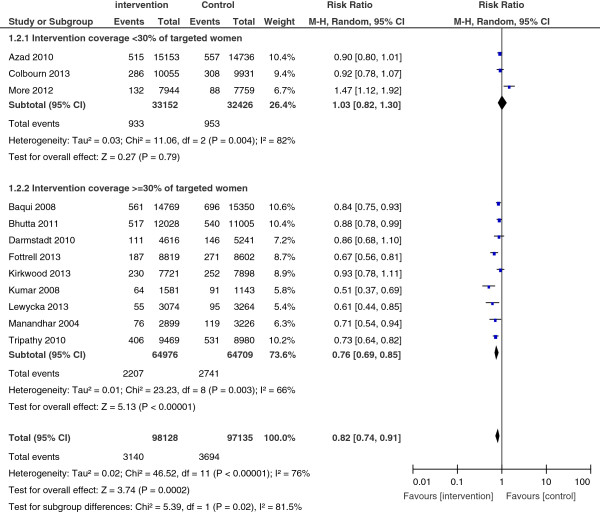
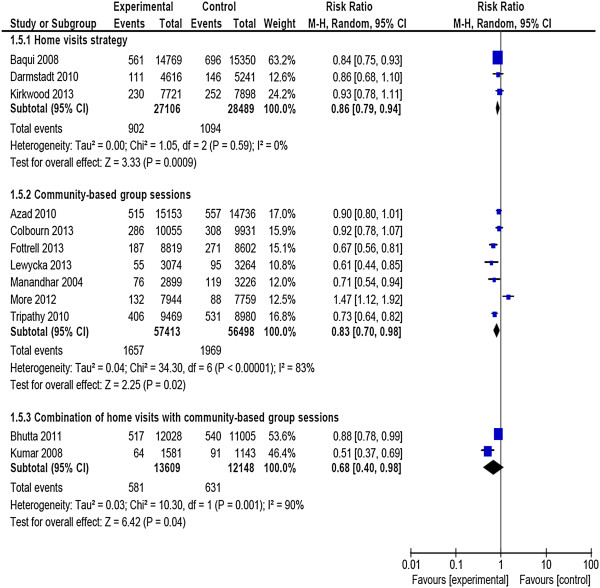
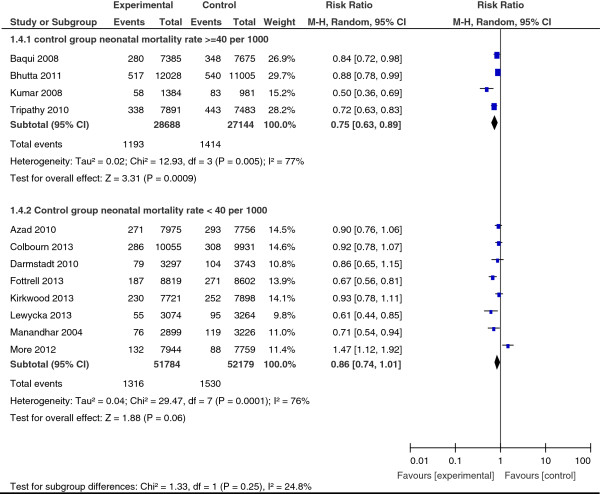
Results: Fourteen randomized studies (292 256 live births) met the inclusion criteria. Meta-analyses showed that exposure to BPCR interventions was associated with a statistically significant reduction of 18% in neonatal mortality risk (twelve studies, RR = 0.82; 95% CI: 0.74, 0.91) and a non-significant reduction of 28% in maternal mortality risk (seven studies, RR = 0.72; 95% CI: 0.46, 1.13). Results were highly heterogeneous (I2 = 76%, p < 0.001 and I2 = 72%, p = 0.002 for neonatal and maternal results, respectively). Subgroup analyses of studies in which at least 30% of targeted women participated in interventions showed a 24% significant reduction of neonatal mortality risk (nine studies, RR = 0.76; 95% CI: 0.69, 0.85) and a 53% significant reduction in maternal mortality risk (four studies, RR = 0.47; 95% CI: 0.26, 0.87).Pooled results revealed that BPCR interventions were also associated with increased likelihood of use of care in the event of newborn illness, clean cutting of the umbilical cord and initiation of breastfeeding in the first hour of life.
Conclusions: With adequate population coverage, BPCR interventions are effective in reducing maternal and neonatal mortality in low-resources settings.
Figures
Comment in
-
Should birth preparedness and complication readiness (BPCR) interventions be scaled up in developing countries?Natl Med J India. 2014 Nov-Dec;27(6):327-8. Natl Med J India. 2014. PMID: 26133331 No abstract available.
References
-
- United Nations. The Millennium Development Goals Report 2012. New York; 2012.
-
- Lozano R, Wang H, Foreman KJ, Rajaratnam JK, Naghavi M, Marcus JR, Dwyer-Lindgren L, Lofgren KT, Phillips D, Atkinson C, Lopez AD, Murray CJ. Progress towards Millennium Development Goals 4 and 5 on maternal and child mortality: an updated systematic analysis. Lancet. 2011;378(9797):1139–1165. doi: 10.1016/S0140-6736(11)61337-8. - DOI - PubMed
-
- Liu L, Johnson HL, Cousens S, Perin J, Scott S, Lawn JE, Rudan I, Campbell H, Cibulskis R, Li M, Mathers C, Black RE. Child Health Epidemiology Reference Group of WHO, Unicef. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379(9832):2151–2161. doi: 10.1016/S0140-6736(12)60560-1. - DOI - PubMed
-
- Barros AJ, Ronsmans C, Axelson H, Loaiza E, Bertoldi AD, Franca GV, Bryce J, Boerma JT, Victora CG. Equity in maternal, newborn, and child health interventions in Countdown to 2015: a retrospective review of survey data from 54 countries. Lancet. 2012;379(9822):1225–1233. doi: 10.1016/S0140-6736(12)60113-5. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
