

Exploring the heterogeneity of effects of corticosteroids on acute respiratory distress syndrome: a systematic review and meta-analysis
- PMID: 24708846
- PMCID: PMC4056095
- DOI: 10.1186/cc13819
Exploring the heterogeneity of effects of corticosteroids on acute respiratory distress syndrome: a systematic review and meta-analysis
Abstract
Introduction: The effectiveness of corticosteroid therapy on the mortality of acute respiratory distress syndrome (ARDS) remains under debate. We aimed to explore the grounds for the inconsistent results in previous studies and update the evidence.
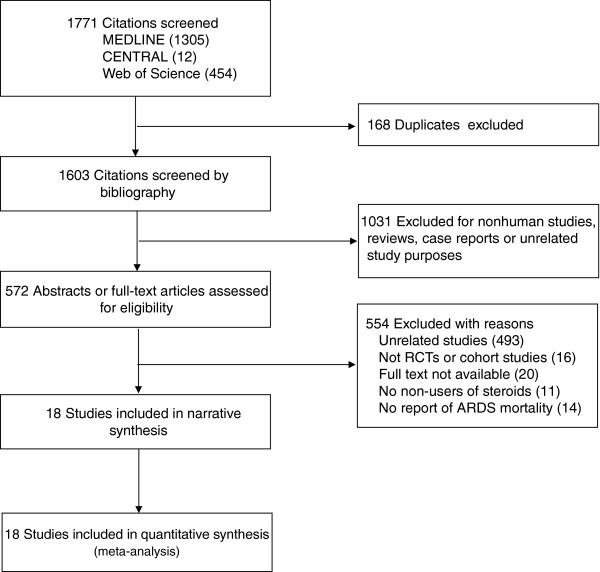
Methods: We searched MEDLINE, Cochrane Central Register of Controlled Trials and Web of Science up to December 2013. Eligible studies included randomized clinical trials (RCTs) and cohort studies that reported mortality and that had corticosteroid nonusers for comparison. The effect of corticosteroids on ARDS mortality was assessed by relative risk (RR) and risk difference (RD) for ICU, hospital, and 60-day mortality using a random-effects model.
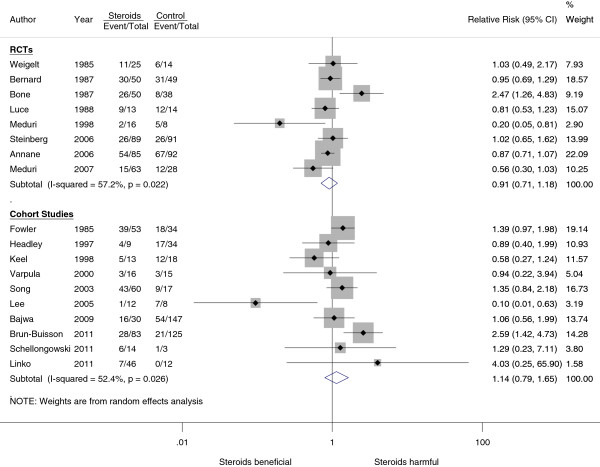
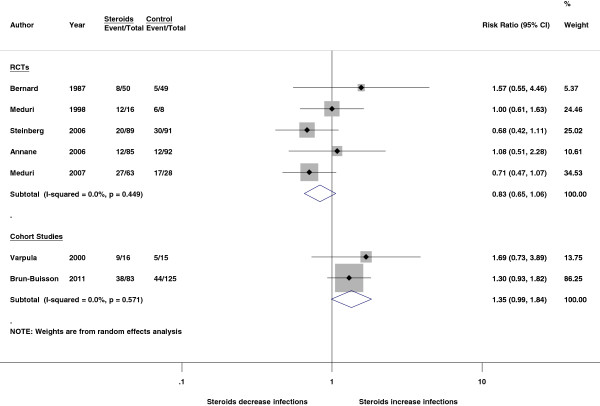
Results: Eight RCTs and 10 cohort studies were included for analysis. In RCTs, corticosteroids had a possible but statistically insignificant effect on ICU mortality (RD, -0.28; 95% confidence interval (CI), -0.53 to -0.03 and RR, 0.55; 95% CI, 0.24 to 1.25) but no effect on 60-day mortality (RD, -0.01; 95% CI, -0.12 to 0.10 and RR, 0.97; 95% CI, 0.75 to 1.26). In cohort studies, corticosteroids had no effect on ICU mortality (RR, 1.05; 95% CI, 0.74 to 1.49) but non-significantly increased 60-day mortality (RR, 1.30; 95% CI, 0.96 to 1.78). In the subgroup analysis by ARDS etiology, corticosteroids significantly increased mortality in influenza-related ARDS (three cohort studies, RR, 2.45, 95% CI, 1.40 to 4.27).
Conclusions: The effects of corticosteroids on the mortality of ARDS differed by duration of outcome measures and etiologies. Corticosteroids did not improve longer-term outcomes and may cause harm in certain subgroups. Current data do not support routine use of corticosteroids in ARDS. More clinical trials are needed to specify the favorable and unfavorable subgroups for corticosteroid therapy.
Figures
Comment in
-
Scandinavian clinical practice guideline on fluid and drug therapy in adults with acute respiratory distress syndrome.Acta Anaesthesiol Scand. 2016 Jul;60(6):697-709. doi: 10.1111/aas.12713. Epub 2016 Mar 14. Acta Anaesthesiol Scand. 2016. PMID: 26988416 Free PMC article. Review.
References
-
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307:2526–2533. - PubMed
-
- Phua J, Badia JR, Adhikari NK, Friedrich JO, Fowler RA, Singh JM, Scales DC, Stather DR, Li A, Jones A, Gattas DJ, Hallett D, Tomlinson G, Stewart TE, Ferguson ND. Has mortality from acute respiratory distress syndrome decreased over time?: a systematic review. Am J Respir Crit Care Med. 2009;179:220–227. doi: 10.1164/rccm.200805-722OC. - DOI - PubMed
-
- Meduri GU, Annane D, Chrousos GP, Marik PE, Sinclair SE. Activation and regulation of systemic inflammation in ARDS: rationale for prolonged glucocorticoid therapy. Chest. 2009;136:1631–1643. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
