

Delay in cART initiation results in persistent immune dysregulation and poor recovery of T-cell phenotype despite a decade of successful HIV suppression
- PMID: 24710051
- PMCID: PMC3977984
- DOI: 10.1371/journal.pone.0094018
Delay in cART initiation results in persistent immune dysregulation and poor recovery of T-cell phenotype despite a decade of successful HIV suppression
Abstract
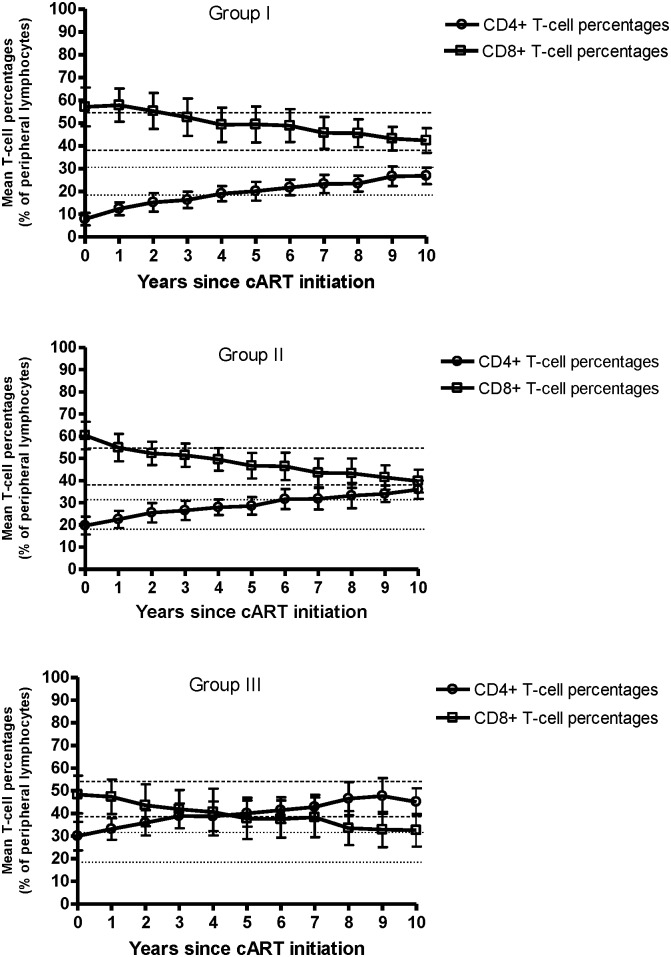
Background: Successful combination antiretroviral therapy (cART) increases levels of CD4+ T-cells, however this increase may not accurately reflect long-term immune recovery since T-cell dysregulation and loss of T-cell homeostasis often persist. We therefore assessed the impact of a decade of effective cART on immune regulation, T-cell homeostasis, and overall T-cell phenotype.
Methods: We conducted a retrospective study of 288 HIV+ cART-naïve patients initiating therapy. We identified 86 individuals who received cART for at least a decade, of which 44 consistently maintained undetectable plasma HIV-RNA levels throughout therapy. At baseline, participants were classified into three groups according to pre-treatment CD4+ T-cell counts: Group I (CD4<200 cells/mm3); Group II (CD4: 200-350 cells/mm3); Group III (CD4>350 cells/mm3). Outcomes of interest were: (1) CD4+ T-cell count restoration (CD4>532 cells/mm3); (2) normalization of CD4:CD8 T-cell ratio (1.2-3.3); (3) maintenance of CD3+ T-cell homeostasis (CD3: 65%-85% of peripheral lymphocytes); (4) normalization of the complete T-cell phenotype (TCP).
Results: Despite a decade of sustained successful cART, complete T-cell phenotype normalization only occurred in 16% of patients, most of whom had initiated therapy at high CD4+ T-cell counts (>350 cells/mm3). The TCP parameter that was the least restored among patients was the CD4:CD8 T-cell ratio.
Conclusions: Failure to normalize the complete T-cell phenotype was most apparent in patients who initiated cART with a CD4+ T-cell count <200 cells/mm3. The impact of this impaired T-cell phenotype on life-long immune function and potential comorbidities remains to be elucidated.
Conflict of interest statement
Figures
References
-
- Stockinger B, Kassiotis G, Bourgeois C (2004) Homeostasis and T cell regulation. Curr Opin Immunol 16: 775–779. - PubMed
-
- Fahey JL, Prince H, Weaver M, Groopman J, Visscher B, et al. (1984) Quantitative changes in T helper or T suppressor/cytotoxic lymphocyte subsets that distinguish acquired immune deficiency syndrome from other immune subset disorders. Am J Med 76: 95–100. - PubMed
-
- Gottlieb MS, Schroff R, Schanker HM, Weisman JD, Fan PT, et al. (1981) Pneumocystis carinii pneumonia and mucosal candidiasis in previously healthy homosexual men: evidence of a new acquired cellular immunodeficiency. N Engl J Med 305: 1425–1431. - PubMed
-
- Malphettes M, Gerard L, Carmagnat M, Mouillot G, Vince N, et al. (2009) Late-onset combined immune deficiency: a subset of common variable immunodeficiency with severe T cell defect. Clin Infect Dis 49: 1329–1338. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
