

Assessment of setup uncertainties for various tumor sites when using daily CBCT for more than 2200 VMAT treatments
- PMID: 24710431
- PMCID: PMC5875470
- DOI: 10.1120/jacmp.v15i2.4418
Assessment of setup uncertainties for various tumor sites when using daily CBCT for more than 2200 VMAT treatments
Abstract
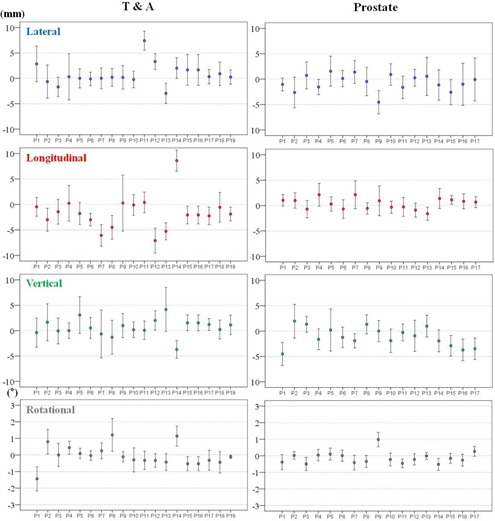
The aim of this study was assess the patient setup errors for various tumor sites based on clinical data from a sufficient number of treatments with volumetric-modulated arc therapy (VMAT) using daily pretreatment CBCT imaging guidance. In addition, we calculated and compared the planning target volume (PTV) margins for all disease sites based on an analysis of specific systematic and random errors in our institution. All patients underwent pretreatment kV-CBCT imaging. The various tumor sites were divided into four categories; 21 brain (438 fractions), 35 head-and-neck tumors (H&N, 933 fractions), 19 thorax and abdomen tumors (T&A, 313 fractions), and 17 prostate cancer tumors (546 fractions). Overall distributions of setup corrections in all directions, frequencies of 3D vector lengths, institution-specific setup error, and PTV margins were analyzed. The longitudinal distribution for the T&A site represented an asymmetric offset in the negative direction. Rotational distributions were comparable for all treatment sites, and the prostate site had the narrowest distribution of ≤ ± 2°. The cumulative frequencies of 3D vector length of ≥ 7 mm were rare for brain lesions and H&N, but more common for T&A and prostate lesions at 25.6% and 12.1%, respectively. The overall mean error for all treatment sites were within ± 1 mm and ± 0.1°, with the exception of the T&A site, which had overall mean error of 2 mm in the negative longitudinal direction. The largest magnitude of systematic error and random error for the brain lesions and H&N was 1.4 mm in the translational directions, and 3.3 mm for T&A and prostate lesions. The PTV margins required in this analysis are ≤ 4 mm for the brain lesions and H&N in all translational directions, but ranged from 4 to 10 mm for T&A and prostate lesions. Analysis of each institution's specific setup errors using daily CBCT is essential for determining PTV margins and reducing setup uncertainties, because setup errors vary according to each immobilization system and patient.
Figures







References
-
- Zietman AL, DeSilvio ML, Slater JD, et al. Comparison of conventional‐dose vs high‐dose conformal radiation therapy in clinically localized adenocarcinoma of the prostate: a randomized controlled trial. JAMA. 2005;294(10):1233–39. - PubMed
-
- Al‐Mamgani A, Heemsbergen WD, Peeters ST, Lebesque JV. Role of intensity‐modulated radiotherapy in reducing toxicity in dose escalation for localized prostate cancer. Int J Radiat Oncol Biol Phys. 2009;73(3):685–91. - PubMed
-
- Fonteyne V, Villeirs G, Speleers B, et al. Intensity‐modulated radiotherapy as primary therapy for prostate cancer: report on acute toxicity after dose escalation with simultaneous integrated boost to intraprostatic lesion. Int J Radiat Oncol Biol Phys. 2008;72(3):799–807. - PubMed
-
- Vora SA, Wong WW, Schild SE, Ezzell GA. Analysis of biochemical control, prognostic factors and toxicities in patients treated with intensity modulated radiotherapy for localized prostate cancer with longer follow‐up. Int J Radiat Oncol Biol Phys. 2008;72(1, Supp):S325–S326. - PubMed
-
- Zelefsky MJ, Fuks Z, Hunt M, et al. High dose radiation delivered by intensity modulated conformal radiotherapy improves the outcome of localized prostate cancer. J Urol. 2001;166(3):876–81. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
