

Regional variation in the correlation of antibody and T-cell responses to Trypanosoma cruzi
- PMID: 24710614
- PMCID: PMC4047731
- DOI: 10.4269/ajtmh.13-0391
Regional variation in the correlation of antibody and T-cell responses to Trypanosoma cruzi
Abstract
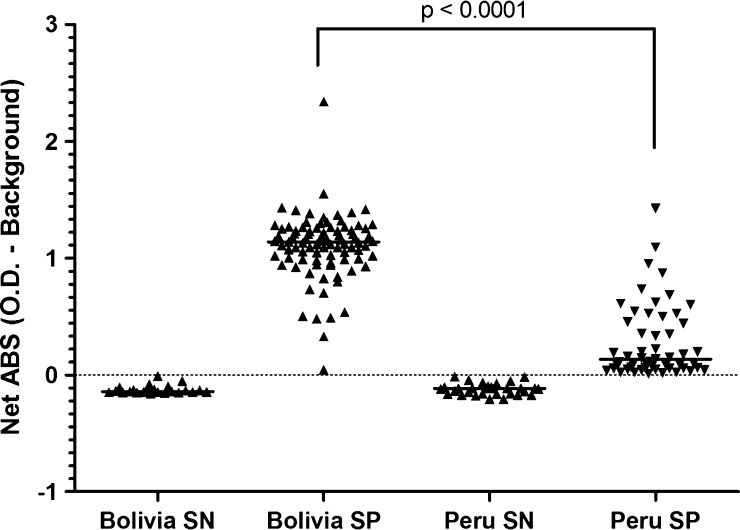
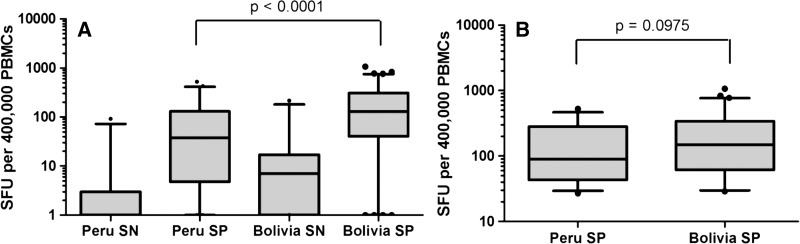
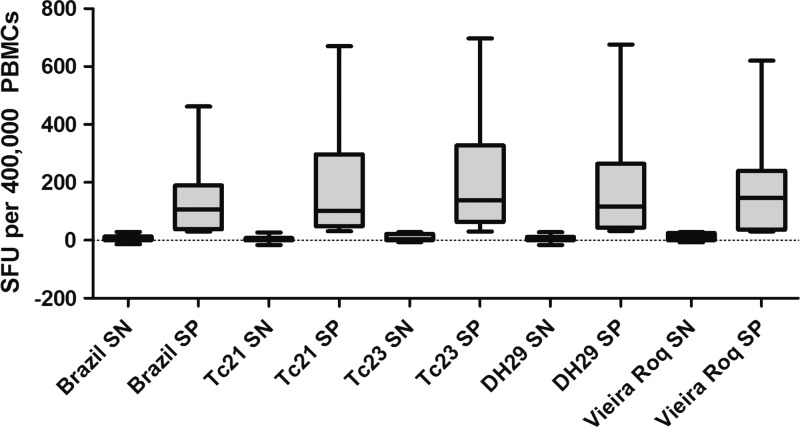
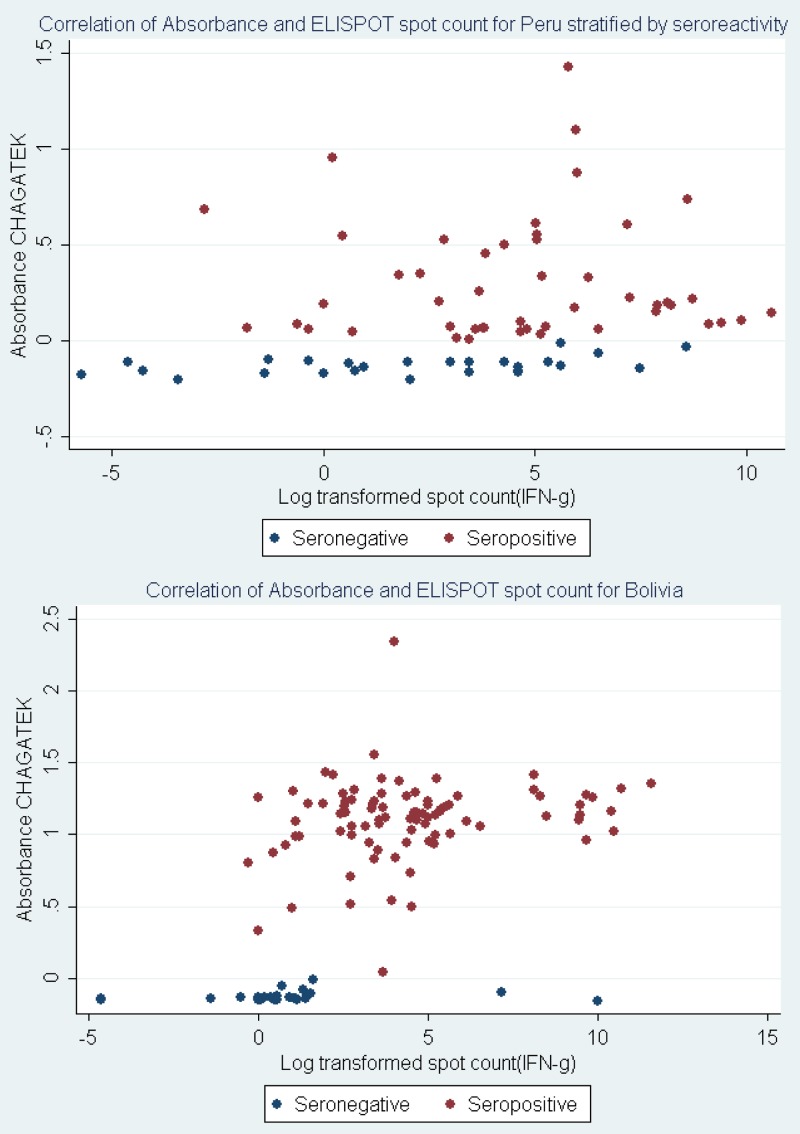
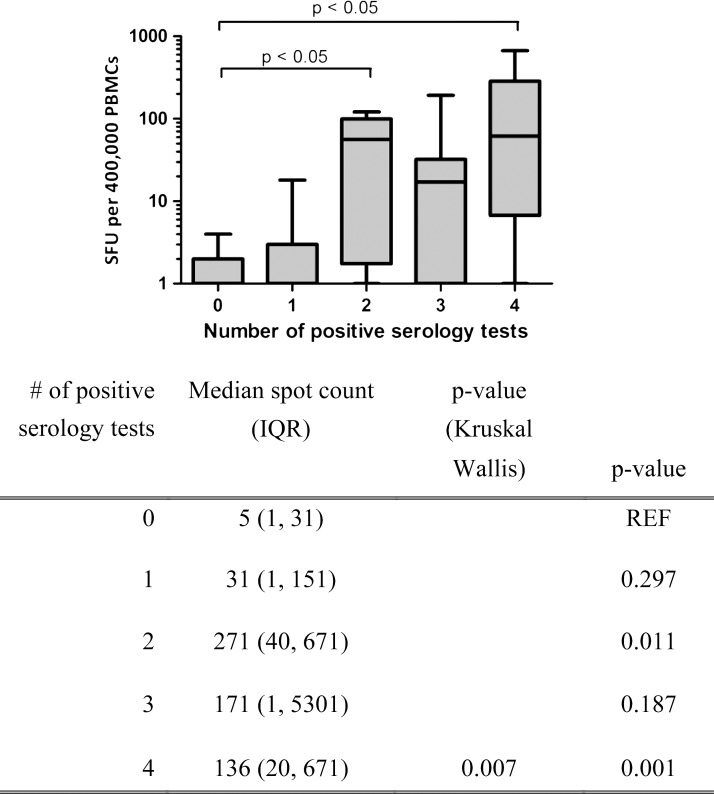
Chagas disease, caused by the protozoan parasite Trypanosoma cruzi, is a major cause of morbidity and mortality in Central and South America. Geographic variations in the sensitivity of serologic diagnostic assays to T. cruzi may reflect differences in T. cruzi exposure. We measured parasite-specific T-cell responses among seropositive individuals in two populations from South America with widely varying antibody titers against T. cruzi. Antibody titers among seropositive individuals were significantly lower in Arequipa, Peru compared with Santa Cruz, Bolivia. Similarly, the proportion of seropositive individuals with positive T-cell responses was lower in Peru than Bolivia, resulting in overall lower frequencies of interferon-γ (IFNγ)-secreting cells from Peruvian samples. However, the magnitude of the IFNγ response was similar among the IFNγ responders in both locations. These data indicate that immunological discrepancies based on geographic region are reflected in T-cell responses as well as antibody responses.
© The American Society of Tropical Medicine and Hygiene.
Figures
References
-
- World Health Organization First WHO Report on Neglected Tropical Diseases: Working to Overcome the Global Impact of Neglected Tropical Disease. 2012. http://whqlibdoc.who.int/publications/2010/9789241564090_eng.pdf Available at. Accessed March 20, 2012.
-
- Schijman AG, Bisio M, Orellana L, Sued M, Duffy T, Mejia Jaramillo AM, Cura C, Auter F, Veron V, Qvarnstrom Y, Deborggraeve S, Hijar G, Zulantay I, Lucero RH, Velazquez E, Tellez T, Sanchez Leon Z, Galvao L, Nolder D, Monje Rumi M, Levi JE, Ramirez JD, Zorrilla P, Flores M, Jercic MI, Crisante G, Anez N, De Castro AM, Gonzalez CI, Acosta Viana K, Yachelini P, Torrico F, Robello C, Diosque P, Triana Chavez O, Aznar C, Russomando G, Buscher P, Assal A, Guhl F, Sosa Estani S, DaSilva A, Britto C, Luquetti A, Ladzins J. International study to evaluate PCR methods for detection of Trypanosoma cruzi DNA in blood samples from Chagas disease patients. PLoS Negl Trop Dis. 2011;5:e931. - PMC - PubMed
-
- Verani JR, Seitz A, Gilman RH, LaFuente C, Galdos-Cardenas G, Kawai V, de LaFuente E, Ferrufino L, Bowman NM, Pinedo-Cancino V, Levy MZ, Steurer F, Todd CW, Kirchhoff LV, Cabrera L, Verastegui M, Bern C. Geographic variation in the sensitivity of recombinant antigen-based rapid tests for chronic Trypanosoma cruzi infection. Am J Trop Med Hyg. 2009;80:410–415. - PubMed
-
- Umezawa ES, Luquetti AO, Levitus G, Ponce C, Ponce E, Henriquez D, Revollo S, Espinoza B, Sousa O, Khan B, da Silveira JF. Serodiagnosis of chronic and acute Chagas' disease with Trypanosoma cruzi recombinant proteins: results of a collaborative study in six Latin American countries. J Clin Microbiol. 2004;42:449–452. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
