

Increasing complexity: which drug class to choose for treatment of hypertension in the elderly?
- PMID: 24711696
- PMCID: PMC3969251
- DOI: 10.2147/CIA.S40154
Increasing complexity: which drug class to choose for treatment of hypertension in the elderly?
Abstract
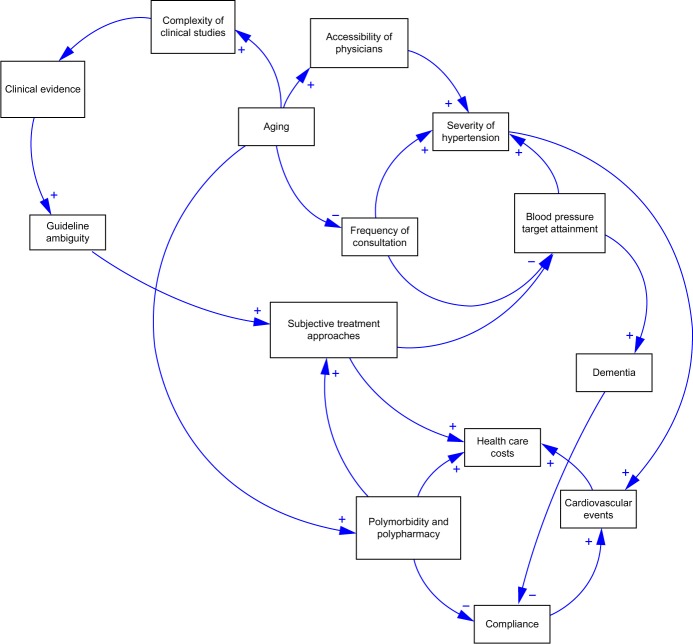
Treatment of hypertension in the elderly is expected to become more complex in the coming decades. Based on the current landscape of clinical trials, guideline recommendations remain inconclusive. The present review discusses the latest evidence derived from studies available in 2013 and investigates optimal blood pressure (BP) and preferred treatment substances. Three common archetypes are discussed that hamper the treatment of hypertension in the very elderly. In addition, this paper presents the current recommendations of the NICE 2011, JNC7 2013-update, ESH/ESC 2013, CHEP 2013, JNC8 and ASH/ISH guidelines for elderly patients. Advantages of the six main substance classes, namely diuretics, beta-blockers (BBs), calcium channel blockers (CCBs), angiotensin-converting enzyme inhibitors (ACEIs), angiotensin receptor blockers (ARBs), and direct renin inhibitors (DRIs) are discussed. Medical and economic implications of drug administration in the very elderly are presented. Avoidance of treatment-related adverse effects has become increasingly relevant. Current substance classes are equally effective, with similar effects on cardiovascular outcomes. Selection of substances should therefore also be based on collateral advantages of drugs that extend beyond BP reduction. The combination of ACEIs and diuretics appears to be favorable in managing systolic/diastolic hypertension. Diuretics are a preferred and cheap combination drug, and the combination with CCBs is recommended for patients with isolated systolic hypertension. ACEIs and CCBs are favorable for patients with dementia, while CCBs and ARBs imply substantial cost savings due to high adherence.
Keywords: antihypertensive therapy; drug; elderly; evidence; guidelines; very elderly.
Figures
References
-
- Simpson FO. Long-term cost and life-expectancy consequences of hypertension. J Hypertens. 1998;16(8):1099–1100. - PubMed
-
- Pimenta E, Oparil S. Management of hypertension in the elderly. Nat Rev Cardiol. 2012;9(5):286–296. - PubMed
-
- Statistisches Bundesamt Bevölkerung Deutschlands bis 2060 12 koordinierte Bevölkerungsvorausberechnung [German population up to 2060 12 Coordinated population projection] 2009. [Accessed February 20, 2014]. Available from https://www.destatis.de/DE/Publikationen/Thematisch/Bevoelkerung/Vorausb....
-
- Aronow WS, Fleg JL, Pepine CJ, et al. ACCF/AHA 2011 expert consensus document on hypertension in the elderly: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents developed in collaboration with the American Academy of Neurology, American Geriatrics Society, American Society for Preventive Cardiology, American Society of Hypertension, American Society of Nephrology, Association of Black Cardiologists, and European Society of Hypertension. J Am Soc Hypertens. 2011;5(4):259–352. - PubMed
-
- Mancia G, Fagard R, Narkiewicz K, et al. Task Force Members 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) J Hypertens. 2013;31(7):1281–1357. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
