

Prevalence and clinical relevance of the morphological substrate of ventricular arrhythmias in patients without known cardiac conditions detected by cardiovascular MR
- PMID: 24712323
- PMCID: PMC4075562
- DOI: 10.1259/bjr.20140059
Prevalence and clinical relevance of the morphological substrate of ventricular arrhythmias in patients without known cardiac conditions detected by cardiovascular MR
Abstract
Objective: Cardiac MR (CMR) identifies the substrate of ventricular arrhythmia (VA) in cardiomyopathies and coronary heart disease. However, little is known about the value of CMR in patients with VA without previously known cardiac disorders.
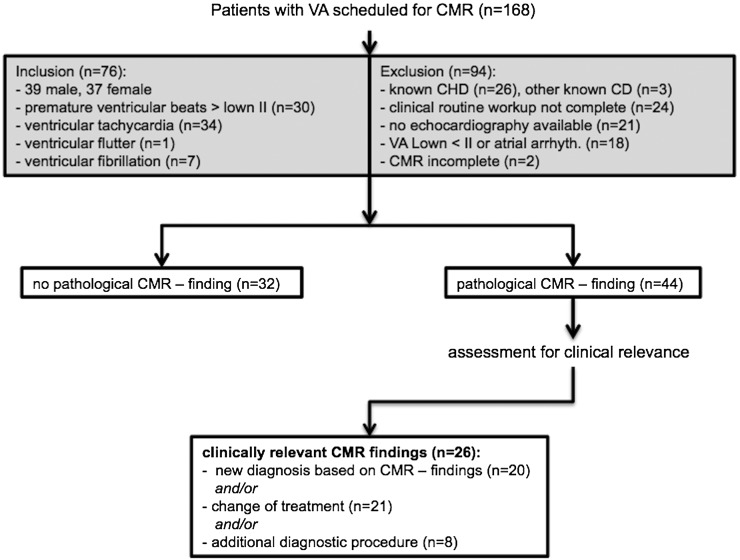
Methods: 76 patients with VA (Lown ≥2) without known cardiac disease after regular diagnostic work-up were studied with CMR, and findings were correlated with electrocardiogram (ECG) and electrophysiological stimulation (EPS). Structural abnormalities matching the VA origin as defined by ECG and/or EPS, or a CMR-detected cardiac condition known to cause arrhythmia were defined as VA substrate. CMR findings were defined as clinically relevant, if resulting in a new diagnosis, change of treatment or additional diagnostic procedure.
Results: 44/76 patients demonstrated pathological CMR findings. In 24/76 patients, the pathology was detected by CMR and not by echocardiography. CMR-based diagnoses of cardiac disease were established in 20/76 patients, and all were morphological substrates for VA. In seven patients, the location of the CMR finding (scar) directly matched the VA origin. CMR findings resulted in a change of treatment in 21 patients and/or additional diagnostics in 8 patients.
Conclusion: Undetected cardiac conditions are frequent causes of VA. This is the first study demonstrating the value of CMR for detection of morphological substrate and/or underlying cardiac disorders in VA patients without known cardiac disease.
Advances in knowledge: The high incidence of clinically relevant CMR findings which were not detected during initial diagnostic work-up strongly supports the use of CMR to screen VA patients for underlying heart disease.
Figures




Similar articles
-
Structural and electrical cardiac abnormalities are prevalent in asymptomatic adults with myotonic dystrophy.Heart. 2016 Sep 15;102(18):1472-8. doi: 10.1136/heartjnl-2015-308517. Epub 2016 May 10. Heart. 2016. PMID: 27164920
-
Electrophysiologic testing for diagnostic evaluation and risk stratification in patients with suspected cardiac sarcoidosis with preserved left and right ventricular systolic function.J Cardiovasc Electrophysiol. 2019 Oct;30(10):1939-1948. doi: 10.1111/jce.14058. Epub 2019 Jul 23. J Cardiovasc Electrophysiol. 2019. PMID: 31257683
-
Screening young athletes for diseases at risk of sudden cardiac death: role of stress testing for ventricular arrhythmias.Eur J Prev Cardiol. 2020 Feb;27(3):311-320. doi: 10.1177/2047487319890973. Epub 2019 Dec 2. Eur J Prev Cardiol. 2020. PMID: 31791144 Free PMC article.
-
Conduction defects/cardiomyopathies.Adv Pediatr. 2014 Aug;61(1):127-48. doi: 10.1016/j.yapd.2014.03.001. Adv Pediatr. 2014. PMID: 25037126 Review. No abstract available.
-
Role of Cardiac Magnetic Resonance Imaging in Patients with Idiopathic Ventricular Arrhythmias.Curr Cardiol Rev. 2019;15(1):12-23. doi: 10.2174/1573403X14666180925095923. Curr Cardiol Rev. 2019. PMID: 30251607 Free PMC article. Review.
Cited by
-
Cardiac Magnetic Resonance to Detect the Underlying Substrate in Patients with Frequent Idiopathic Ventricular Arrhythmias.Diagnostics (Basel). 2021 Jun 18;11(6):1109. doi: 10.3390/diagnostics11061109. Diagnostics (Basel). 2021. PMID: 34207123 Free PMC article.
-
Role of Cardiac Magnetic Resonance in the Assessment of Patients with Premature Ventricular Contractions: A Narrative Review.Anatol J Cardiol. 2024 Jun 4;28(10):467-78. doi: 10.14744/AnatolJCardiol.2024.4314. Online ahead of print. Anatol J Cardiol. 2024. PMID: 38832526 Free PMC article.
References
-
- Boye P, Abdel-Aty H, Zacharzowsky U, Bohl S, Schwenke C, van der Geest RJ, et al. . Prediction of life-threatening arrhythmic events in patients with chronic myocardial infarction by contrast-enhanced CMR. JACC Cardiovasc Imaging 2011; 4: 871–9. - PubMed
-
- Moon JC, McKenna WJ, McCrohon JA, Elliott PM, Smith GC, Pennell DJ. Toward clinical risk assessment in hypertrophic cardiomyopathy with gadolinium cardiovascular magnetic resonance. J Am Coll Cardiol 2003; 41: 1561–7. - PubMed
-
- Yan AT, Shayne AJ, Brown KA, Gupta SN, Chan CW, Luu TM, et al. . Characterization of the peri-infarct zone by contrast-enhanced cardiac magnetic resonance imaging is a powerful predictor of post-myocardial infarction mortality. Circulation 2006; 114: 32–9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
