

Evaluation of patterns of liver toxicity in patients on antiretroviral and anti-tuberculosis drugs: a prospective four arm observational study in ethiopian patients
- PMID: 24714066
- PMCID: PMC3979833
- DOI: 10.1371/journal.pone.0094271
Evaluation of patterns of liver toxicity in patients on antiretroviral and anti-tuberculosis drugs: a prospective four arm observational study in ethiopian patients
Abstract
Objectives: To evaluate the incidence, type, severity and predictors of antiretroviral and/or anti-tuberculosis drugs induced liver injury (DILI).
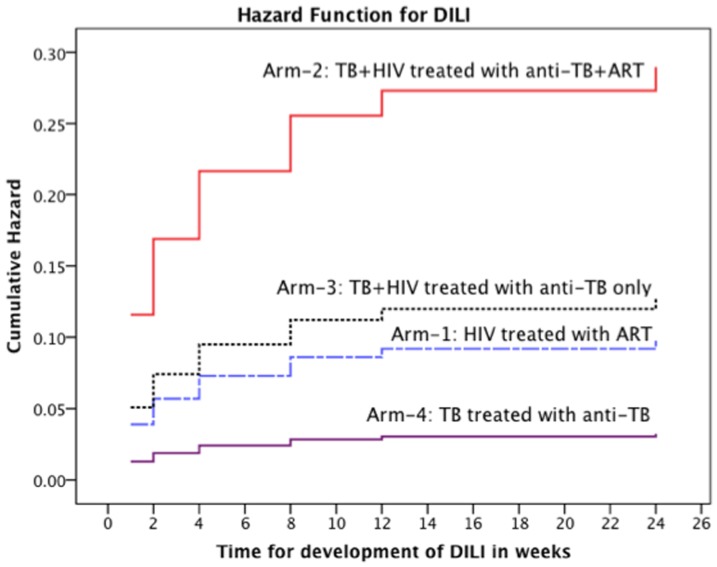
Methods: A total of 1,060 treatment naive patients were prospectively enrolled into four treatment groups: HIV patients receiving efavirenz based HAART alone (Arm-1); TB-HIV co-infected patients with CD4≤200 cells/μL, receiving concomitant rifampicin based anti-TB and efavirenz based HAART (Arm-2); TB-HIV co-infected patients with CD4>200 cells/μL, receiving anti-TB alone (Arm-3); TB patients taking rifampicin based anti-TB alone (Arm-4). Liver enzyme levels were monitored at baseline, 1st, 2nd, 4th, 8th, 12th and 24th weeks during treatment. CD4 and HIV viral load was measured at baseline, 24th and 48th weeks. Data were analyzed using multivariate Cox Proportional Hazards Model.
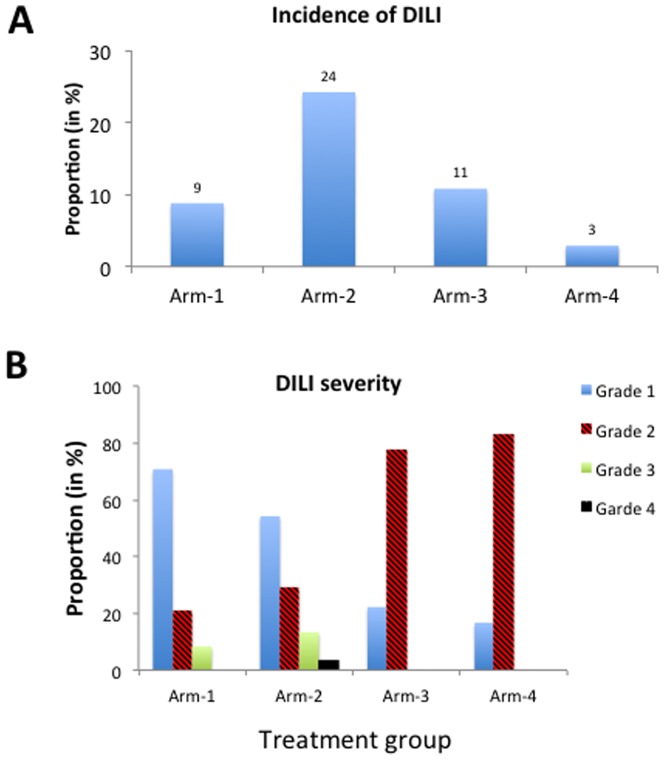
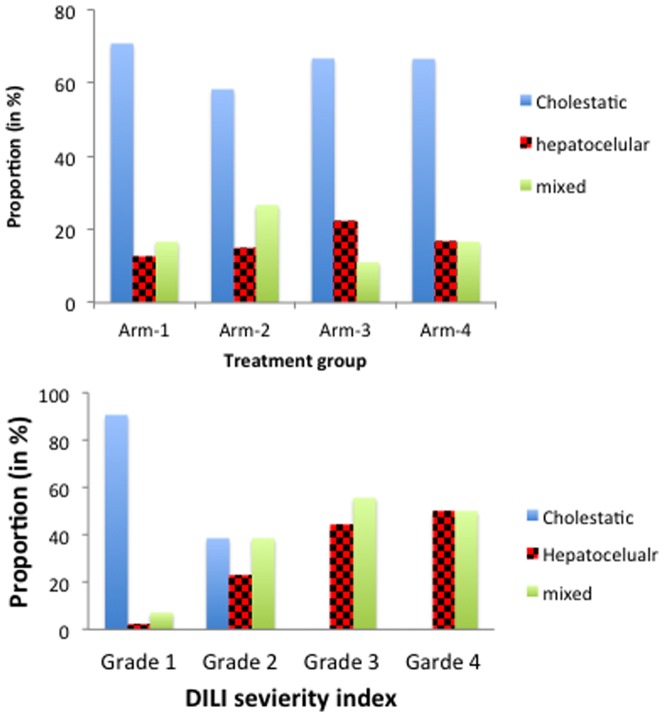
Results: A total of 159 patients (15%) developed DILI with severity grades 1, 2, 3 and 4 of 53.5%, 32.7%, 11.3% and 2.5% respectively. The incidence of cholestatic, hepatocellular or mixed pattern was 61%, 15% and 24%, respectively. Incidence of DILI was highest in Arm-2 (24.2%)>Arm-3 (10.8%)>Arm-1 (8.8%)>Arm-4 (2.9%). Concomitant anti-TB-HIV therapy increased the risk of DILI by 10-fold than anti-TB alone (p<0.0001). HIV co-infection increased the risk of anti-TB DILI by 4-fold (p = 0.004). HAART associated DILI was 3-fold higher than anti-TB alone, (p = 0.02). HAART was associated with cholestatic and grade 1 DILI whereas anti-TB therapy was associated with hepatocellular and grade ≥ 2. Treatment type, lower CD4, platelet, hemoglobin, higher serum AST and direct bilirubin levels at baseline were significant DILI predictors. There was no effect of DILI on immunologic recovery or virologic suppression rate of HAART.
Conclusion: HAART associated DILI is mainly cholestatic and mild whereas hepatocellular or mixed pattern with high severity grade is more common in anti-tuberculosis DILI. TB-HIV co-infection, disease severity and concomitant treatment exacerbates the risk of DILI.
Conflict of interest statement
Figures
References
-
- Walker UA (2007) Antiretroviral therapy-induced liver alterations. Curr Opin HIV AIDS 2: 293–298. - PubMed
-
- Reisler RB, Han C, Burman WJ, Tedaldi EM, Neaton JD (2003) Grade 4 events are as important as AIDS events in the era of HAART. J Acquir Immune Defic Syndr 34: 379–386. - PubMed
-
- Nunez M (2010) Clinical syndromes and consequences of antiretroviral-related hepatotoxicity. Hepatology 52: 1143–1155. - PubMed
-
- Inductivo-Yu I, Bonacini M (2008) Highly active antiretroviral therapy-induced liver injury. Curr Drug Saf 3: 4–13. - PubMed
-
- Tostmann A, Boeree MJ, Aarnoutse RE, de Lange WC, van der Ven AJ, et al. (2008) Antituberculosis drug-induced hepatotoxicity: concise up-to-date review. J Gastroenterol Hepatol 23: 192–202. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
