

The anatomy of primary care and mental health clinician communication: a quality improvement case study
- PMID: 24715400
- PMCID: PMC4070235
- DOI: 10.1007/s11606-013-2731-7
The anatomy of primary care and mental health clinician communication: a quality improvement case study
Abstract
Background: The high prevalence of comorbid physical and mental illnesses among veterans is well known. Therefore, ensuring effective communication between primary care (PC) and mental health (MH) clinicians in the Veterans Affairs (VA) health care system is essential. The VA's Patient Aligned Care Teams (PACT) initiative has further raised awareness of the need for communication between PC and MH. Improving such communication, however, has proven challenging.
Objective: To qualitatively understand barriers to PC-MH communication in an academic community-based clinic by using continuous quality improvement (CQI) tools and then initiate a change strategy.
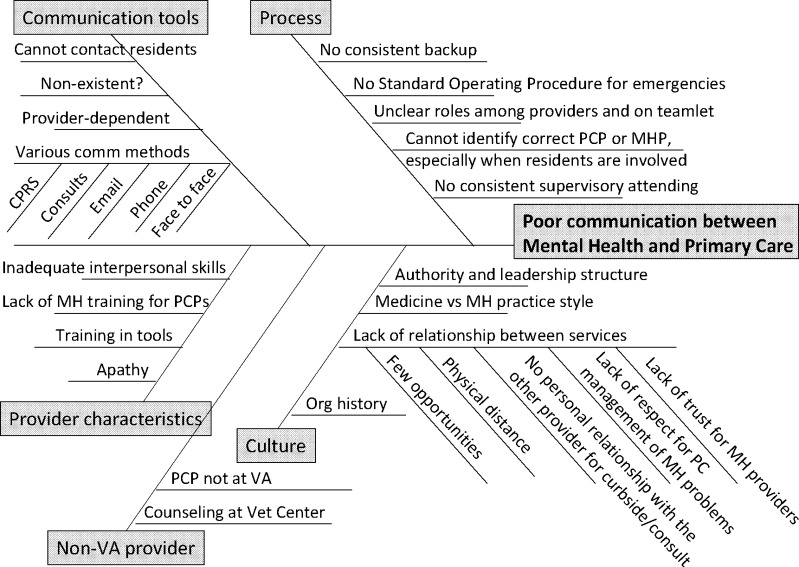
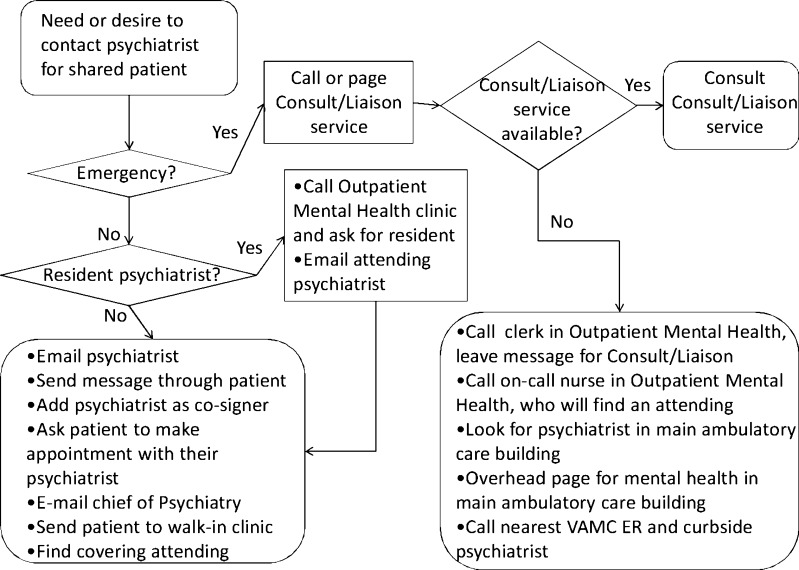
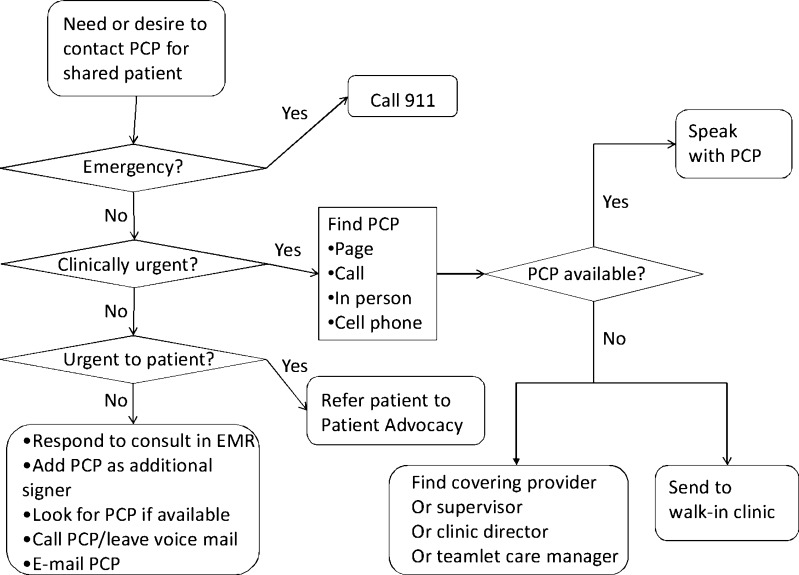
Design, participants, and approach: An interdisciplinary quality improvement (QI) work group composed of 11 on-site PC and MH providers, administrators, and researchers identified communication barriers and facilitators using fishbone diagrams and process flow maps. The work group then verified and provided context for the diagram and flow maps through medical record review (32 patients who received both PC and MH care), interviews (6 stakeholders), and reports from four previously completed focus groups. Based on these findings and a previous systematic review of interventions to improve interspecialty communication, the team initiated plans for improvement.
Key results: Key communication barriers included lack of effective standardized communication processes, practice style differences, and inadequate PC training in MH. Clinicians often accessed advice or formal consultation based on pre-existing across-discipline personal relationships. The work group identified collocated collaborative care, joint care planning, and joint case conferences as feasible, evidence-based interventions for improving communication.
Conclusions: CQI tools enabled providers to systematically assess local communication barriers and facilitators and engaged stakeholders in developing possible solutions. A locally tailored CQI process focusing on communication helped initiate change strategies and ongoing improvement efforts.
Figures
Similar articles
-
Impact of Evidence-Based Quality Improvement on Tailoring VA's Patient-Centered Medical Home Model to Women Veterans' Needs.J Gen Intern Med. 2024 Jun;39(8):1349-1359. doi: 10.1007/s11606-024-08647-4. Epub 2024 Feb 29. J Gen Intern Med. 2024. PMID: 38424344 Free PMC article. Clinical Trial.
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Veterans' mental health beliefs: Facilitators and barriers to primary care-mental health use.Fam Syst Health. 2016 Dec;34(4):404-413. doi: 10.1037/fsh0000231. Epub 2016 Nov 7. Fam Syst Health. 2016. PMID: 27819439
-
[Charisma and leadership: new challenges for psychiatry].Encephale. 2013 Dec;39(6):445-51. doi: 10.1016/j.encep.2012.10.006. Epub 2012 Dec 13. Encephale. 2013. PMID: 23246329 Review. French.
-
Stroke Inpatient Rehabilitation Team Conferences: Leadership and Structure Improve Patient Outcomes.J Stroke Cerebrovasc Dis. 2020 Apr;29(4):104622. doi: 10.1016/j.jstrokecerebrovasdis.2019.104622. Epub 2020 Feb 6. J Stroke Cerebrovasc Dis. 2020. PMID: 32037267 Review.
Cited by
-
Transitioning patients from outpatient mental health services to primary care: A rapid literature review.Implement Res Pract. 2021 Sep 14;2:26334895211041294. doi: 10.1177/26334895211041294. eCollection 2021 Jan-Dec. Implement Res Pract. 2021. PMID: 37089993 Free PMC article. Review.
-
Patient experiences with a primary care medical home tailored for people with serious mental illness.Fam Syst Health. 2024 Jun;42(2):214-225. doi: 10.1037/fsh0000853. Epub 2023 Nov 13. Fam Syst Health. 2024. PMID: 37956066 Free PMC article.
-
Random or predictable?: Adoption patterns of chronic care management practices in physician organizations.Implement Sci. 2017 Aug 24;12(1):106. doi: 10.1186/s13012-017-0639-z. Implement Sci. 2017. PMID: 28836996 Free PMC article.
-
Perspectives of Migrant Youth, Parents and Clinicians on Community-Based Mental Health Services: Negotiating Safe Pathways.J Child Fam Stud. 2017;26(7):1936-1948. doi: 10.1007/s10826-017-0700-1. Epub 2017 Mar 27. J Child Fam Stud. 2017. PMID: 28680260 Free PMC article.
-
Japanese family physicians' attitudes, difficulties, and perceived significance in managing mental health problems: A qualitative study.J Gen Fam Med. 2024 Sep 16;26(1):37-44. doi: 10.1002/jgf2.731. eCollection 2025 Jan. J Gen Fam Med. 2024. PMID: 39776870 Free PMC article.
References
-
- Yoon J, Yano E, Altman L, et al. Reducing costs of acute care for ambulatory case-sensitive medical conditions: the central roles of comorbid mental illness. Med Care. 2012. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
