

Role of neuroimaging in HIV-associated neurocognitive disorders
- PMID: 24715492
- PMCID: PMC4217280
- DOI: 10.1055/s-0034-1372346
Role of neuroimaging in HIV-associated neurocognitive disorders
Abstract
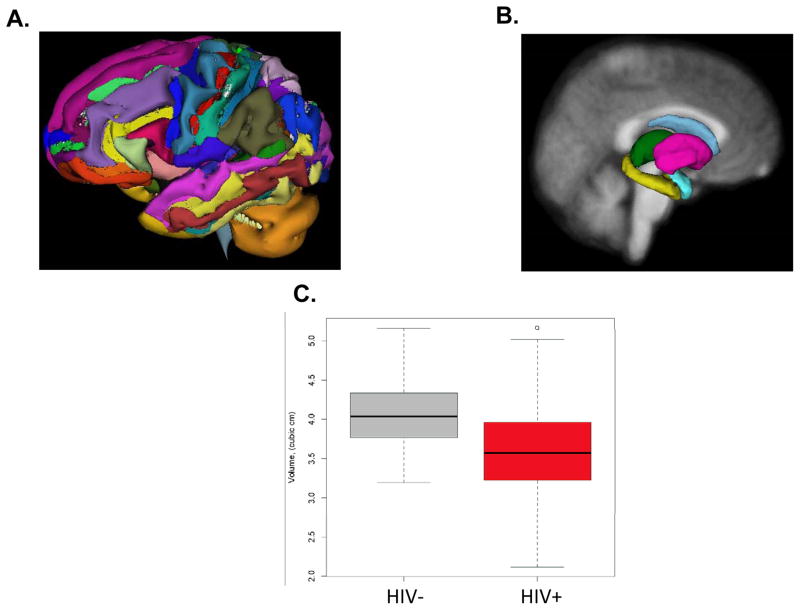
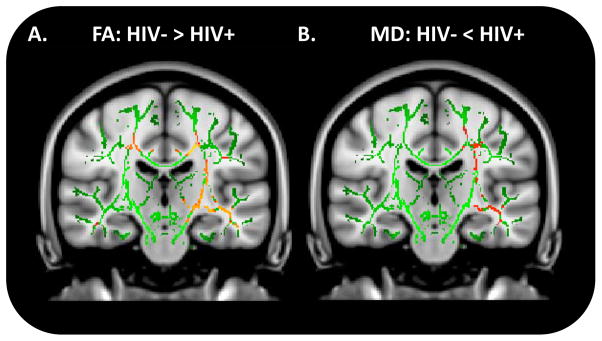
Human immunodeficiency virus (HIV) enters the brain soon after seroconversion and can cause HIV-associated neurocognitive disorders (HAND). Although the more severe and progressive forms of HAND are less prevalent due to combination antiretroviral therapy (cART), ∼ 40% of HIV-infected (HIV+) patients continue to have cognitive impairment. Some HIV+ individuals who have effective plasma HIV-1 RNA suppression with cART still develop HAND. It is often difficult to diagnose HAND in the outpatient setting as detailed neuropsychological performance testing is required. Additional biomarkers that are relatively easy to obtain and clinically relevant are needed for assessing HIV-associated neuropathologic changes. Recently developed noninvasive magnetic resonance imaging (MRI) techniques have great potential to serve as biomarkers. The authors review the application of some of these neuroimaging techniques, magnetic resonance spectroscopy (MRS), volumetric MRI, diffusion tensor imaging (DTI), functional MRI (fMRI), in HIV+ individuals. Each of the neuroimaging methods offers unique insight into mechanisms underlying neuroHIV, could monitor disease progression, and may assist in evaluating the efficacy of particular cART regimens. It is hoped that considerable progress will continue to occur such that some of these neuroimaging methods will be incorporated across multiple sites and included in future HAND guidelines.
Thieme Medical Publishers 333 Seventh Avenue, New York, NY 10001, USA.
Figures
References
-
- Justice AC. HIV and aging: time for a new paradigm. Current HIV/AIDS reports. 2010 May;7(2):69–76. - PubMed
-
- Aberg JA, Kaplan JE, Libman H, et al. Primary care guidelines for the management of persons infected with human immunodeficiency virus: 2009 update by the HIV medicine Association of the Infectious Diseases Society of America. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America. 2009 Sep 1;49(5):651–681. - PubMed
-
- Luther VP, Wilkin AM. HIV infection in older adults. Clinics in geriatric medicine. 2007 Aug;23(3):567–583. vii. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
