

Evaluation of computer-assisted mandibular reconstruction with vascularized iliac crest bone graft compared to conventional surgery: a randomized prospective clinical trial
- PMID: 24716651
- PMCID: PMC3998950
- DOI: 10.1186/1745-6215-15-114
Evaluation of computer-assisted mandibular reconstruction with vascularized iliac crest bone graft compared to conventional surgery: a randomized prospective clinical trial
Abstract
Background: Computer-assisted surgery plays an increasingly important role in mandibular reconstruction, ensuring the best possible masticatory function and aesthetic outcome.
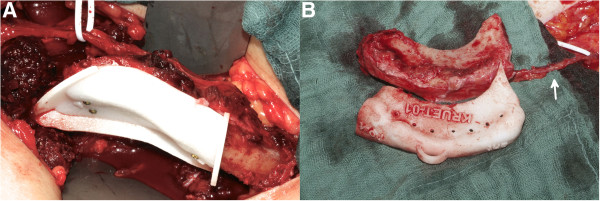
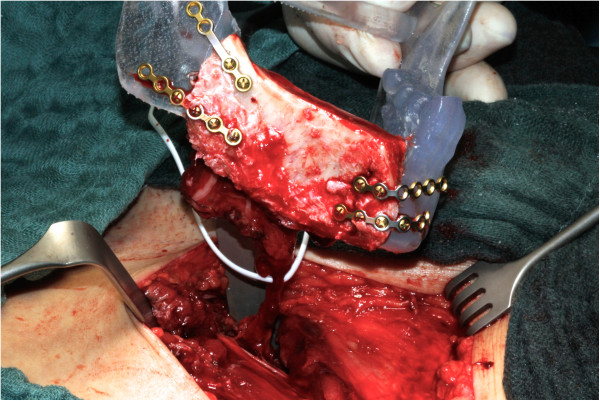
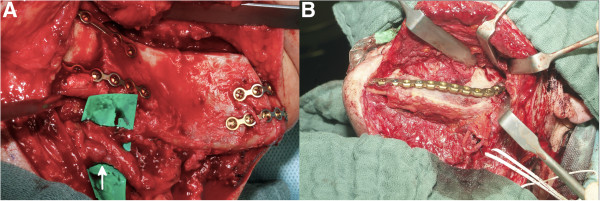
Methods: Twenty patients were randomly assigned to computer-assisted or conventional mandibular reconstruction with vascularized iliac crest bone graft in a prospective study design.Virtual surgical planning was based on preoperative CT-data using specific surgical planning software. A rapid prototyping guide transferred the virtual surgery plan to the operation site. During surgery the transplant ischemic time, reconstruction time, time for shaping the transplant and amount of bone removed were measured. Additionally, the difference in the intercondylar distance before and after surgery was calculated.
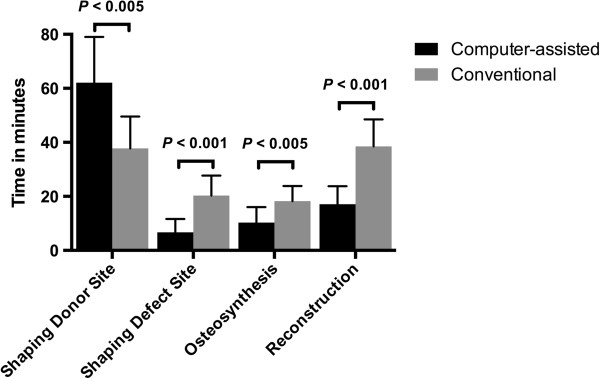
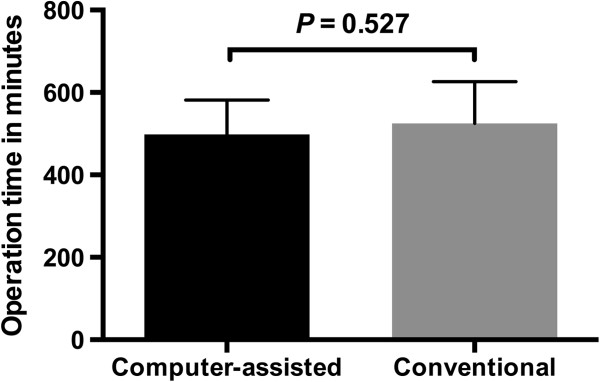
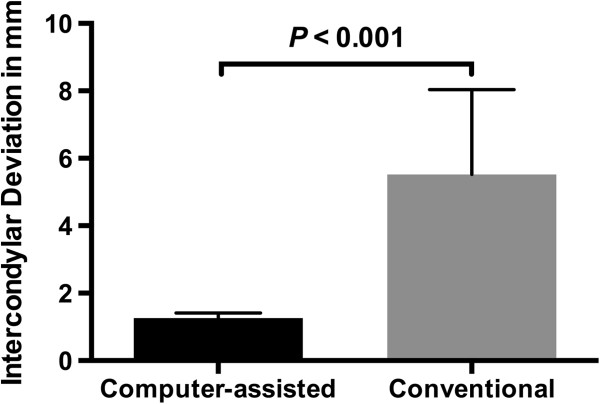
Results: Computer-assisted surgery shortened the time of transplant ischemia (P < 0.005) and defect reconstruction (P < 0.001) compared to conventional surgery. The time to saw and shape the transplant at the donor site was shorter using conventional surgery (P < 0.005); therefore, the overall time for surgery didn't change (P = 0.527). In the computer-assisted group, the amount of bone harvested equaled the defect size, whereas the transplant size in the conventional group exceeded the defect site by 16.8 ± 5.6 mm (P < 0.001) on average. The intercondylar distance before compared to after surgery was less affected in the computer-assisted than in the conventional group (P < 0.001).
Conclusions: The presented study shows that computer-assisted surgery can help reduce the time for mandibular defect reconstruction and consequently the transplant ischemic time. In the computer-assisted group, the iliac crest donor site defect was downsized and the postoperative condyle position was less altered, reducing possible risks of postoperative complications and donor site morbidity.
Trial registration: DRKS00005181.
Figures





References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
