

Should chloride-rich crystalloids remain the mainstay of fluid resuscitation to prevent 'pre-renal' acute kidney injury?: con
- PMID: 24717302
- PMCID: PMC4255073
- DOI: 10.1038/ki.2014.105
Should chloride-rich crystalloids remain the mainstay of fluid resuscitation to prevent 'pre-renal' acute kidney injury?: con
Abstract
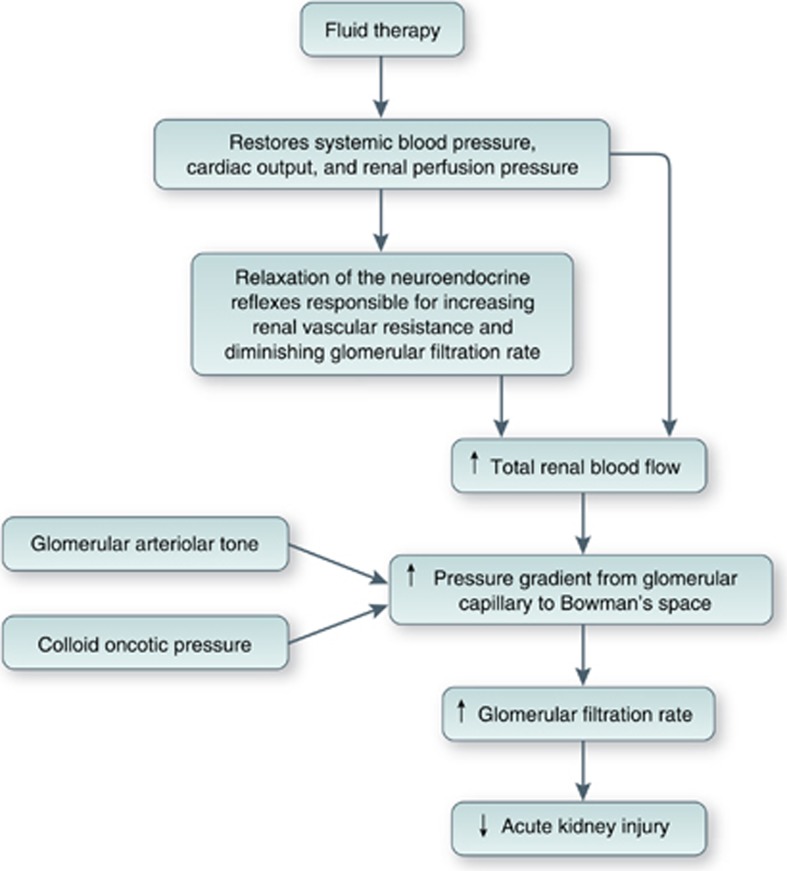
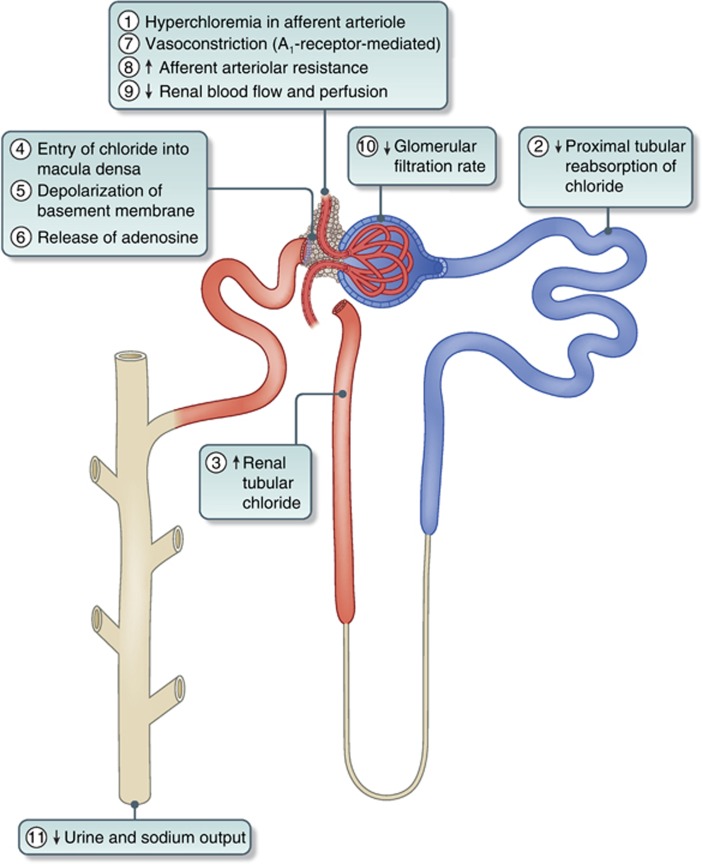
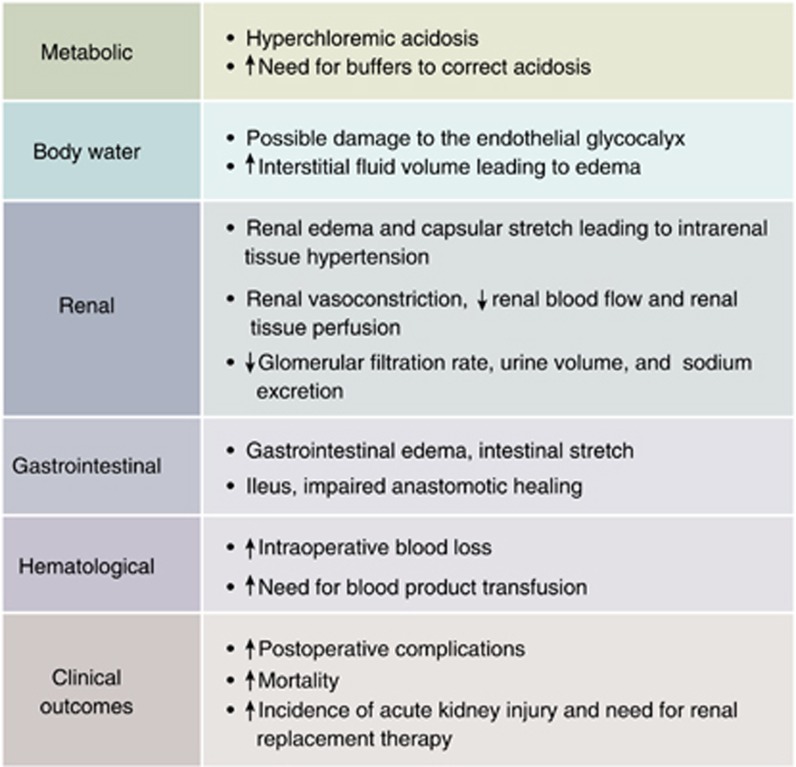
The high chloride content of 0.9% saline leads to adverse pathophysiological effects in both animals and healthy human volunteers, changes not seen after balanced crystalloids. Small randomized trials confirm that the hyperchloremic acidosis induced by saline also occurs in patients, but no clinical outcome benefit was demonstrable when compared with balanced crystalloids, perhaps due to a type II error. A strong signal is emerging from recent large propensity-matched and cohort studies for the adverse effects that 0.9% saline has on the clinical outcome in surgical and critically ill patients when compared with balanced crystalloids. Major complications are the increased incidence of acute kidney injury and the need for renal replacement therapy, and that pathological hyperchloremia may increase postoperative mortality. However, there are no large-scale randomized trials comparing 0.9% saline with balanced crystalloids. Some balanced crystalloids are hypo-osmolar and may not be suitable for neurosurgical patients because of their propensity to cause brain edema. Saline may be the solution of choice used for the resuscitation of patients with alkalosis and hypochloremia. Nevertheless, there is evidence to suggest that balanced crystalloids cause less detriment to renal function than 0.9% saline, with perhaps better clinical outcome. Hence, we argue that chloride-rich crystalloids such as 0.9% saline should be replaced with balanced crystalloids as the mainstay of fluid resuscitation to prevent 'pre-renal' acute kidney injury.
Figures
References
-
- Evans GH. The abuse of normal salt solution. JAMA. 1911;57:2126–2127.
-
- Wakim KG. ‘‘Normal'' 0.9 per cent salt solution is neither ‘‘normal'' nor physiological. JAMA. 1970;214:1710. - PubMed
-
- Reid F, Lobo DN, Williams RN, et al. (Ab)normal saline and physiological Hartmann's solution: a randomized double-blind crossover study. Clin Sci (Lond) 2003;104:17–24. - PubMed
-
- Prowle JR, Bellomo R. Fluid administration and the kidney. Curr Opin Crit Care. 2010;16:332–336. - PubMed
-
- Lobo DN. Sir David Cuthbertson medal lecture. Fluid, electrolytes and nutrition: physiological and clinical aspects. Proc Nutr Soc. 2004;63:453–466. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
