

Does incorporation of thromboelastography improve bleeding prediction following adult cardiac surgery?
- PMID: 24717423
- PMCID: PMC4162333
- DOI: 10.1097/MBC.0000000000000095
Does incorporation of thromboelastography improve bleeding prediction following adult cardiac surgery?
Abstract
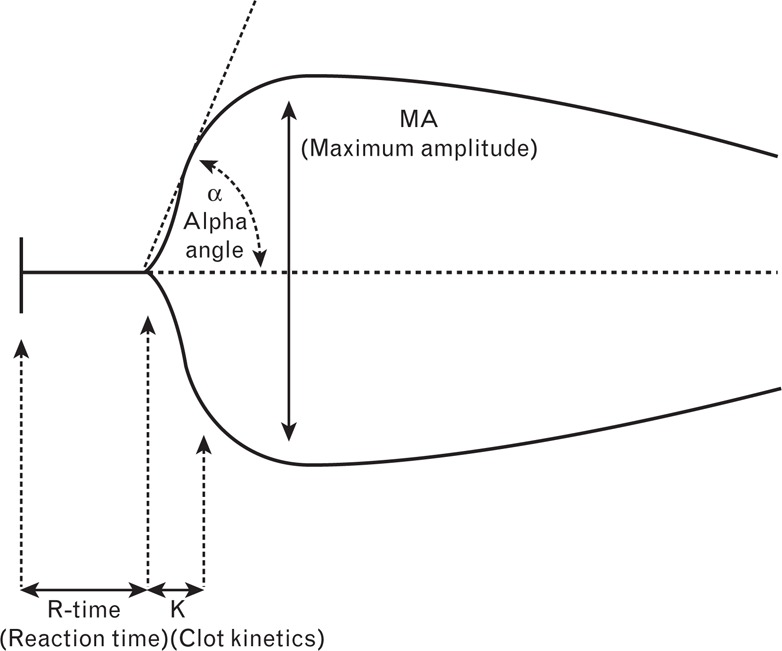
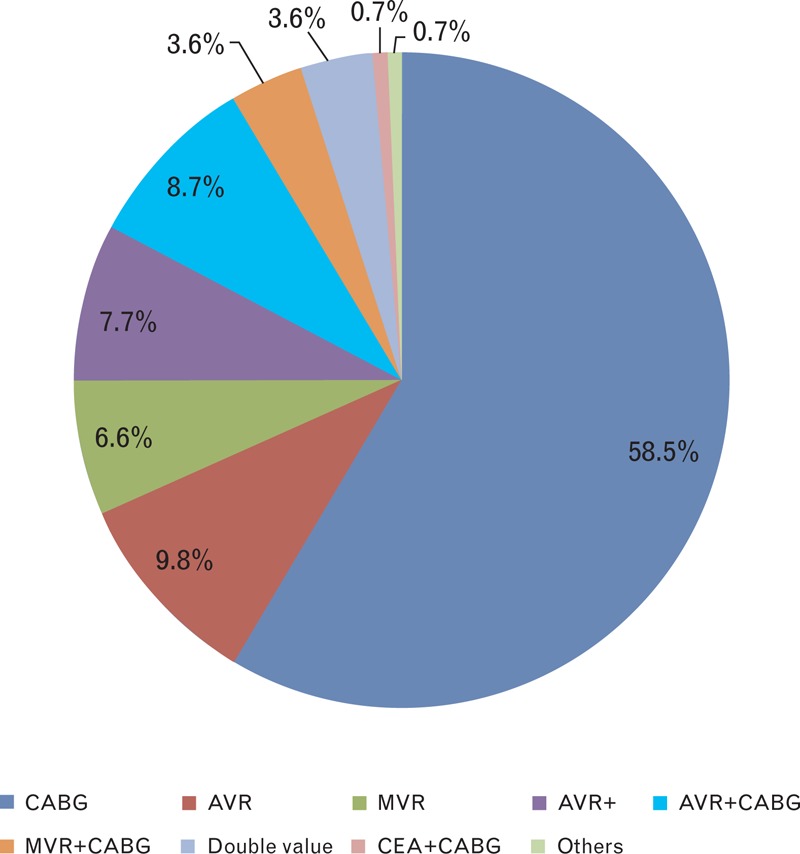
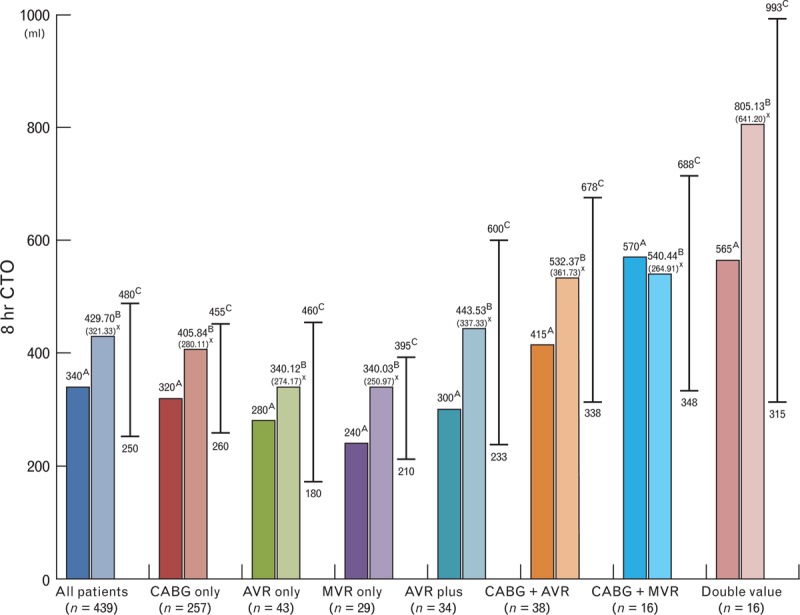
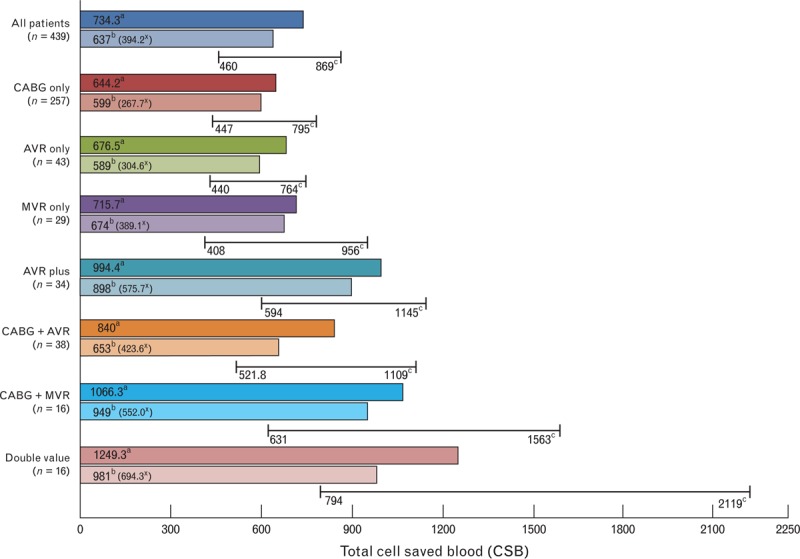
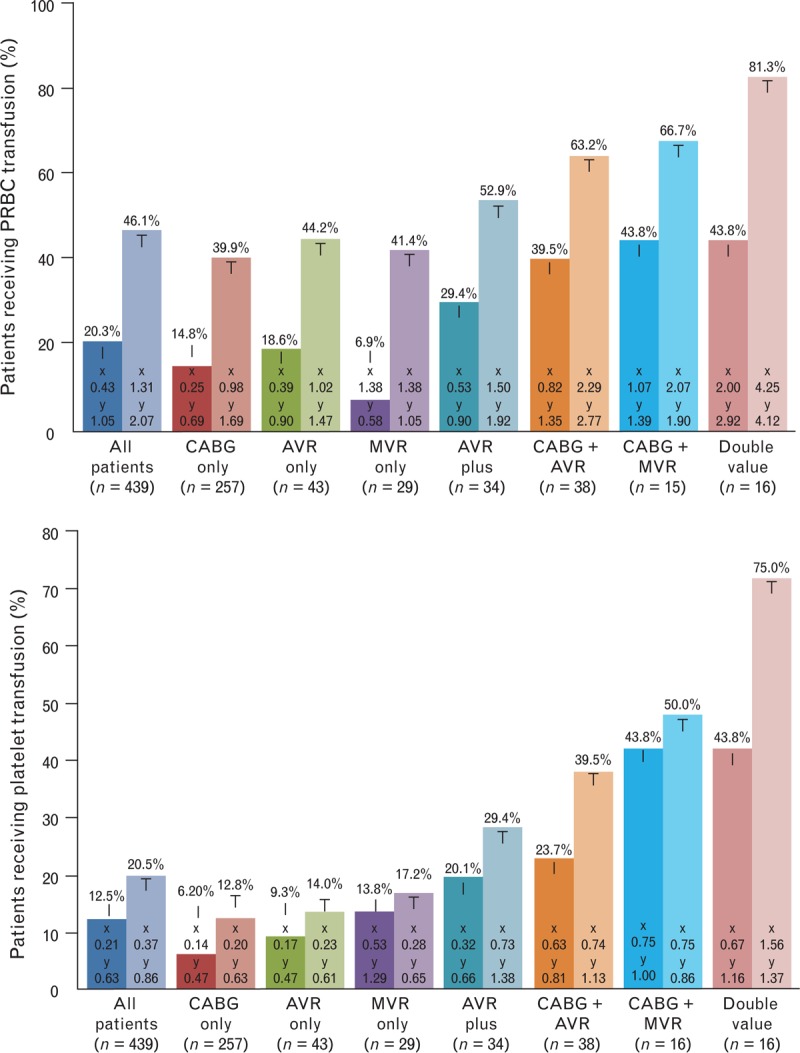
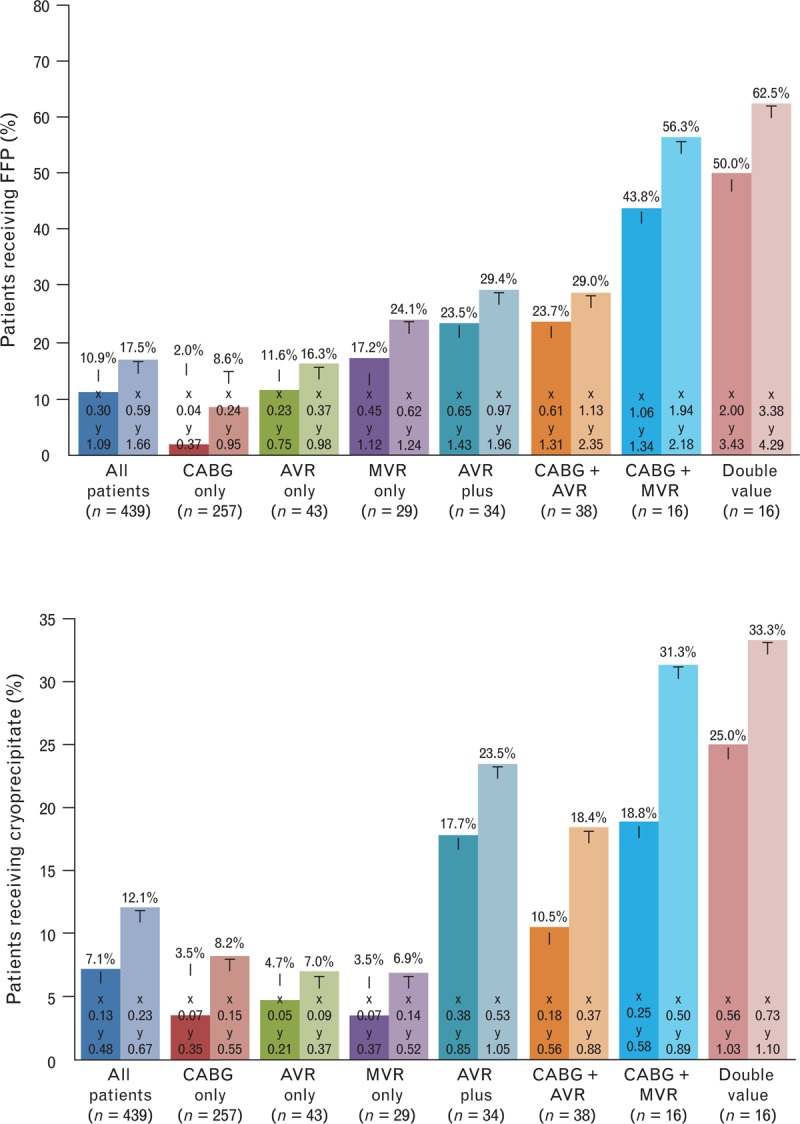
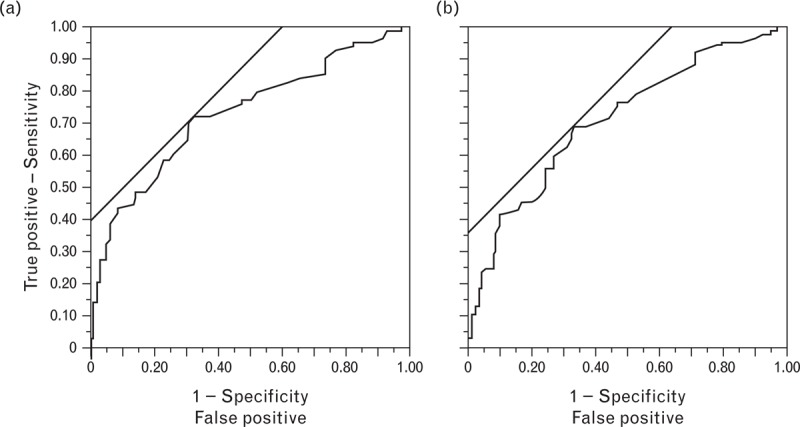
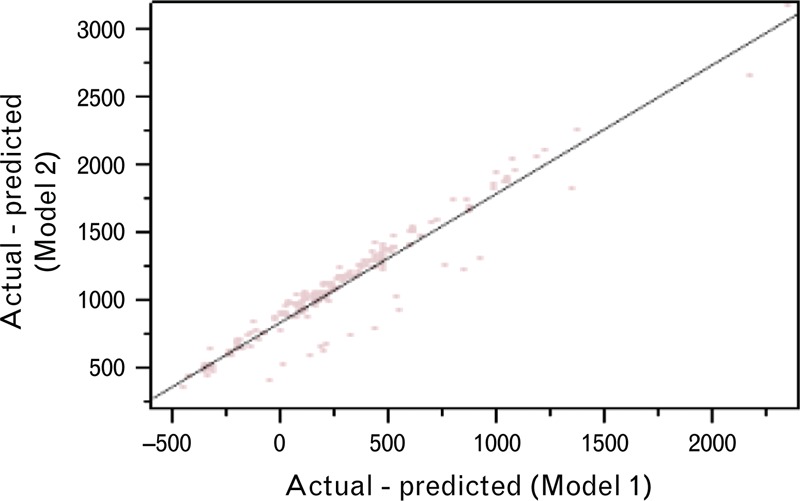
Cardiopulmonary bypass (CPB) coagulopathy increases utilization of allogenic blood/blood products, which can negatively affect patient outcomes. Thromboelastography (TEG) is a point-of-care measurement of clot formation and fibrinolysis. We investigated whether the addition of TEG parameters to a clinically based bleeding model would improve the predictability of postoperative bleeding. A total of 439 patients' charts were retrospectively investigated for 8-h chest tube output (CTO) postoperatively. For model 1, the variables recorded were patient age, gender, body surface area, clopidogrel use, CPB time, first post-CPB fibrinogen serum level, first post-CPB platelet count, first post-CPB international normalized ratio, the total amount of intraoperative cell saver blood transfused, and postoperative first ICU hematocrit level. Model 2 had the model 1 variables, TEG angle, and maximum amplitude. The outcome was defined as 0-8-h CTO. The predictor variables were placed into a forward stepwise regression model for continuous outcomes. Analysis of variance with adjusted R was used to assess the goodness-of-fit of both predictive models. The predictive accuracy of the model was examined using CTO as a dichotomous variable (75th percentile, 480 ml) and receiver operating characteristic curves for both models. Advanced age, male gender, preoperative clopidogrel use for 5 days or less, greater cell saver blood utilization, and lower postoperative hematocrit levels were associated with increased 8-h CTO (P < 0.05). Adding TEG angle and maximum amplitude to model 1 did not improve CTO predictability. When TEG angle and maximum amplitude were added as predictor factors, the predictability of the bleeding model did not improve.
Figures
Comment in
-
Thrombelastography will not predict bleeding if normal.Blood Coagul Fibrinolysis. 2015 Mar;26(2):234. doi: 10.1097/MBC.0000000000000195. Blood Coagul Fibrinolysis. 2015. PMID: 25629422 No abstract available.
Similar articles
-
Does rotational thromboelastometry (ROTEM) improve prediction of bleeding after cardiac surgery?Anesth Analg. 2012 Sep;115(3):499-506. doi: 10.1213/ANE.0b013e31825e7c39. Epub 2012 Jun 19. Anesth Analg. 2012. PMID: 22713683
-
Thromboelastograph with Platelet Mapping(TM) predicts postoperative chest tube drainage in patients undergoing coronary artery bypass grafting.J Cardiothorac Vasc Anesth. 2014 Apr;28(2):217-23. doi: 10.1053/j.jvca.2013.12.010. J Cardiothorac Vasc Anesth. 2014. PMID: 24630471
-
Comparison between thromboelastography and conventional coagulation tests after cardiopulmonary bypass surgery in the paediatric intensive care unit.Int J Lab Hematol. 2014 Aug;36(4):465-71. doi: 10.1111/ijlh.12171. Epub 2013 Dec 11. Int J Lab Hematol. 2014. PMID: 24325756
-
Thromboelastography and cardiopulmonary bypass.Semin Thromb Hemost. 1995;21 Suppl 4:27-33. Semin Thromb Hemost. 1995. PMID: 8747685 Review.
-
A systematic review of thromboelastography utilization in vascular and endovascular surgery.J Vasc Surg. 2022 Mar;75(3):1107-1115. doi: 10.1016/j.jvs.2021.11.037. Epub 2021 Nov 14. J Vasc Surg. 2022. PMID: 34788649
Cited by
-
Thromboelastography after Cardiopulmonary Bypass: Does it Save Blood Products?Kans J Med. 2022 Jan 11;15(1):27-30. doi: 10.17161/kjm.vol15.15789. eCollection 2022. Kans J Med. 2022. PMID: 35106120 Free PMC article.
-
Should viscoelastic testing be a standard point-of-care test on all intensive care units?J Intensive Care Soc. 2024 Oct 15;25(4):432-439. doi: 10.1177/17511437241290154. eCollection 2024 Nov. J Intensive Care Soc. 2024. PMID: 39524069 Free PMC article. Review.
-
Utility of thromboelastography versus routine coagulation tests for assessment of hypocoagulable state in patients undergoing cardiac bypass surgery.Ann Card Anaesth. 2018 Apr-Jun;21(2):151-157. doi: 10.4103/aca.ACA_174_17. Ann Card Anaesth. 2018. PMID: 29652276 Free PMC article.
-
Comparison of Thromboelastography and Conventional Coagulation Tests in Patients With Severe Liver Disease.Clin Appl Thromb Hemost. 2020 Jan-Dec;26:1076029620925915. doi: 10.1177/1076029620925915. Clin Appl Thromb Hemost. 2020. PMID: 32496878 Free PMC article.
-
Point-of-care viscoelastic testing.BJA Educ. 2022 Nov;22(11):416-423. doi: 10.1016/j.bjae.2022.07.003. Epub 2022 Sep 2. BJA Educ. 2022. PMID: 36304915 Free PMC article. Review. No abstract available.
References
-
- Goodnough LT, Soegiarso RW, Birkmeyer JD, Welch HG. Economic impact of inappropriate blood transfusions in coronary artery bypass graft surgery. Am J Med 1993; 94:509–514 - PubMed
-
- Hendrickson JE, Hillyer CD. Noninfectious serious hazards of transfusion. Anesth Analg 2009; 108:759–769 - PubMed
-
- Johansson PI, Sølbeck S, Genet G, Stensballe J, Ostrowski SR. Coagulopathy and hemostatic monitoring in cardiac surgery: an update. Scand Cardiovasc J 2012; 46:194–202 - PubMed
-
- Ferraris VA, Ferraris SP, Saha SP, Hessel EA, 2nd, Haan CK, Royston BD, et al. Perioperative blood transfusion and blood conservation in cardiac surgery: the Society of Thoracic Surgeons and the Society of Cardiovascular Anesthesiologists Clinical Practice Guideline. Ann Thorac Surg 2007; 83:S27–S86 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
