

Sedation, sleep promotion, and delirium screening practices in the care of mechanically ventilated children: a wake-up call for the pediatric critical care community*
- PMID: 24717461
- PMCID: PMC4061156
- DOI: 10.1097/CCM.0000000000000326
Sedation, sleep promotion, and delirium screening practices in the care of mechanically ventilated children: a wake-up call for the pediatric critical care community*
Abstract
Objectives: To examine pediatric intensivist sedation management, sleep promotion, and delirium screening practices for intubated and mechanically ventilated children.
Design: An international, online survey of questions regarding sedative and analgesic medication choices and availability, sedation protocols, sleep optimization, and delirium recognition and treatment.
Setting: Member societies of the World Federation of Pediatric Intensive and Critical Care Societies were asked to send the survey to their mailing lists; responses were collected from July 2012 to January 2013.
Subjects: Pediatric critical care providers.
Interventions: Survey.
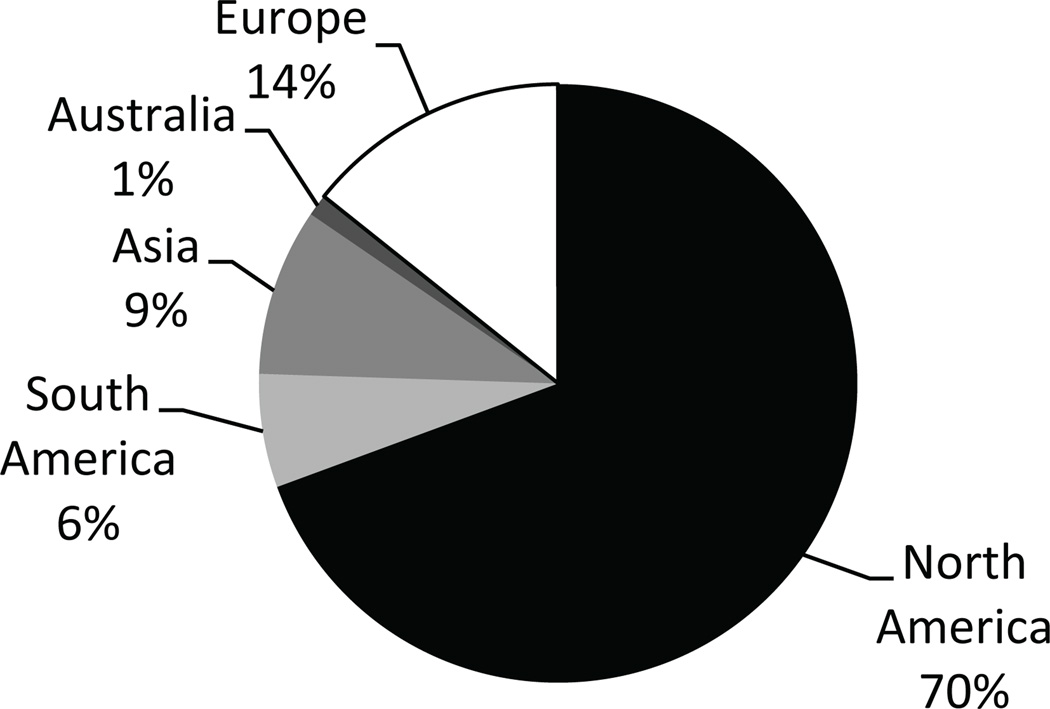
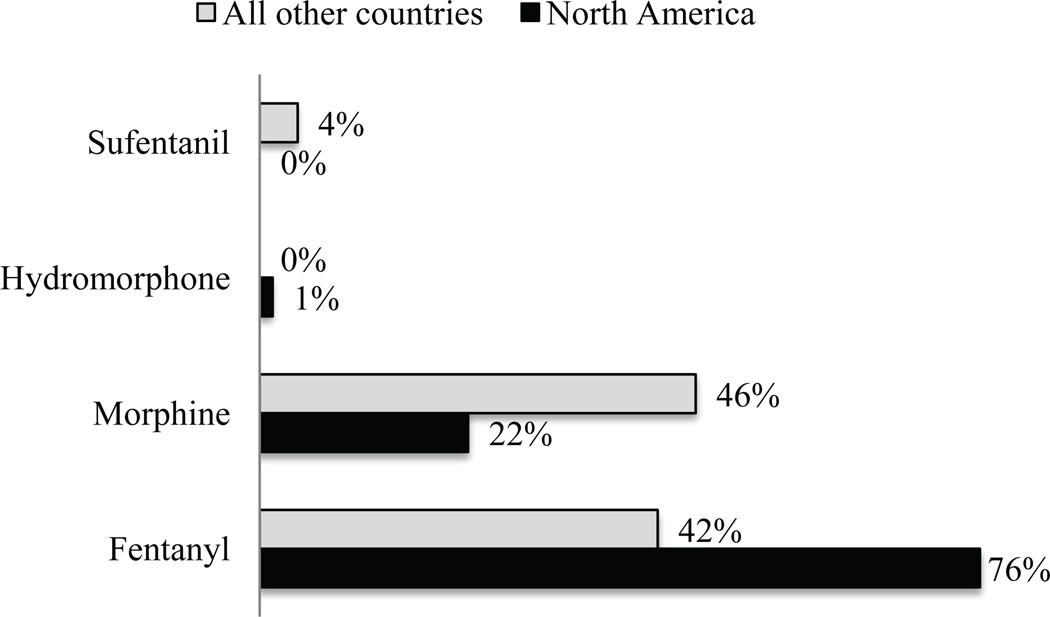
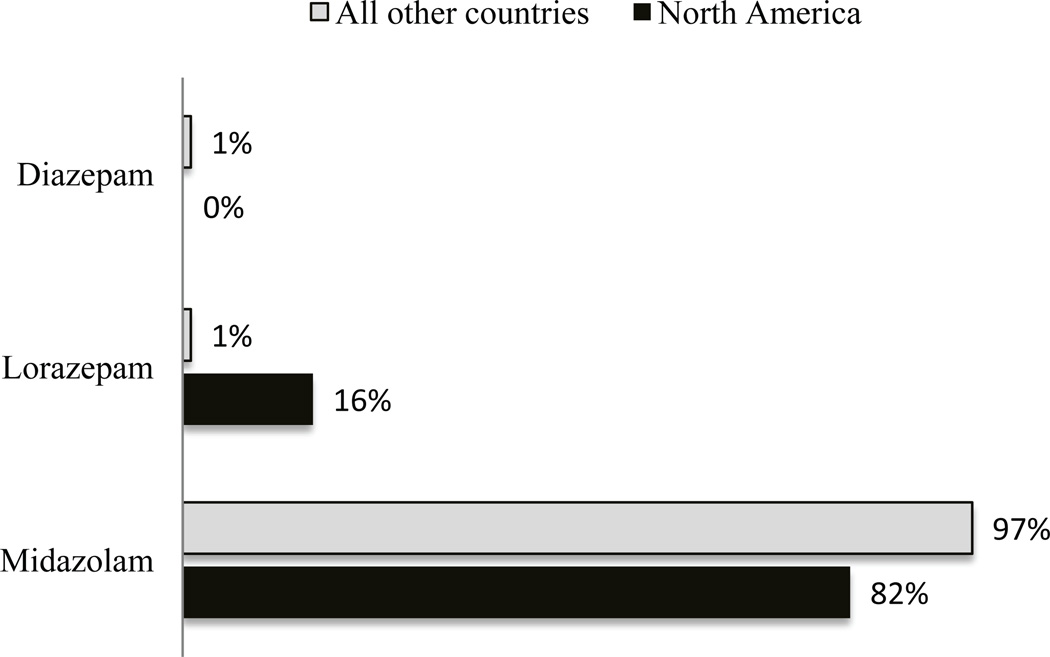
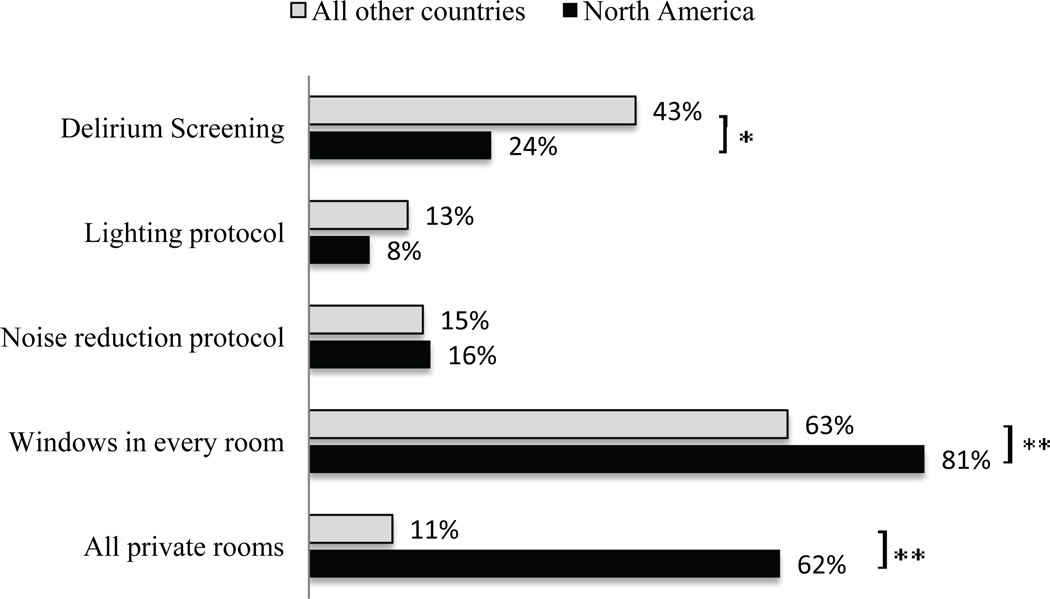
Measurements and main results: The survey was completed by 341 respondents, the majority of whom were from North America (70%). Twenty-seven percent of respondents reported having written sedation protocols. Most respondents worked in PICUs with sedation scoring systems (70%), although only 42% of those with access to scoring systems reported routine daily use for goal-directed sedation management. The State Behavioral Scale was the most commonly used scoring system in North America (22%), with the COMFORT score more prevalent in all other countries (39%). The most commonly used sedation regimen for intubated children was a combination of opioid and benzodiazepine (72%). Most intensivists chose fentanyl as their first-line opioid (66%) and midazolam as their first-line benzodiazepine (86%) and prefer to administer these medications as continuous infusions. Propofol and dexmedetomidine were the most commonly restricted medications in PICUs internationally. Use of earplugs, eye masks, noise reduction, and lighting optimization for sleep promotion was uncommon. Delirium screening was not practiced in 71% of respondent's PICUs, and only 2% reported routine screening at least twice a day.
Conclusions: The results highlight the heterogeneity in sedation practices among intensivists who care for critically ill children as well as a paucity of sleep promotion and delirium screening in PICUs worldwide.
Figures
Comment in
-
On the lack of standardized essential PICU guidelines*.Crit Care Med. 2014 Jul;42(7):1724-5. doi: 10.1097/CCM.0000000000000367. Crit Care Med. 2014. PMID: 24933046 No abstract available.
References
-
- Kudchadkar S, Sterni L, Yaster M, Easley RB. Sleep in the Intensive Care Unit. Contemporary Critical Care. 2009;7:1–12.
-
- Friese RS. Sleep and recovery from critical illness and injury: A review of theory, current practice, and future directions. Crit Care Med. 2008;36:697–705. - PubMed
-
- Pandharipande P, Shintani A, Peterson J, et al. Lorazepam is an independent risk factor for transitioning to delirium in intensive care unit patients. Anesthesiology. 2006;104:21–26. - PubMed
-
- Aydogan MS, Korkmaz MF, Ozgül U, et al. Pain, fentanyl consumption, and delirium in adolescents after scoliosis surgery: dexmedetomidine vs midazolam. Paediatr Anaesth. 2013;23(5):446–452. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
