

Individuality of the plasma sodium concentration
- PMID: 24717732
- PMCID: PMC4059970
- DOI: 10.1152/ajprenal.00585.2013
Individuality of the plasma sodium concentration
Abstract
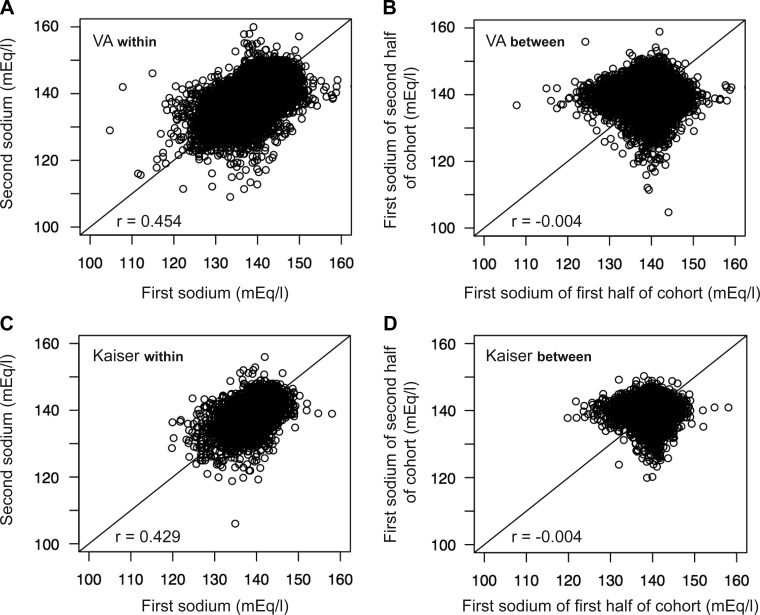
Older literature has suggested that the plasma sodium concentration is not individual, that it is neither intrinsic to an individual nor reproducible, longitudinally. We recently observed that the plasma sodium concentration is heritable. Because demonstrable heritability requires individuality of the relevant phenotype, we hypothesized that the plasma sodium concentration was substantially individual. In two large health plan-based cohorts, we demonstrated individuality of the plasma sodium concentration over a 10-yr interval; the intraclass correlation coefficient (ICC) averaged 0.4-0.5. The individuality of plasma sodium increased significantly with age. Plasma sodium individuality was equal to or only slightly less than that for plasma glucose but was less than the individuality for creatinine. The individuality of plasma sodium was further confirmed by comparing the Pearson correlation coefficient for within-individual versus between-individual pairs of sodium determinations and via application of the agreement index. Furthermore, the distribution of all sodium determinations for all participants within a population was similar to the distribution for the mean sodium concentration for individuals within that population. Therefore, the near-normal distribution of plasma sodium measurements within a population is likely not attributable to assay-specific factors but rather to genuine and durable biological variability in the osmotic set point. In aggregate, these data strongly support the individuality of the plasma sodium concentration. They further indicate that serial plasma sodium values for any given individual tend to cluster around a patient-specific set point and that these set points vary among individuals.
Keywords: human; hyponatremia; osmoregulation; population.
Figures









Comment in
-
New insights into the determinants of serum Na+ and the risk for dysnatremias.Am J Physiol Renal Physiol. 2014 Jul 1;307(1):F12-3. doi: 10.1152/ajprenal.00217.2014. Epub 2014 May 7. Am J Physiol Renal Physiol. 2014. PMID: 24808532 No abstract available.
References
-
- Adrogue HJ, Madias NE. Hyponatremia. N Engl J Med 342: 1581–1589, 2000 - PubMed
-
- Allison SP, Lobo DN. Fluid and electrolytes in the elderly. Curr Opin Clin Nutr Metab Care 7: 27–33, 2004 - PubMed
-
- Ayus JC, Arieff AI. Abnormalities of water metabolism in the elderly. Semin Nephrol 16: 277–288, 1996 - PubMed
-
- Barr EL, Boyko EJ, Zimmet PZ, Wolfe R, Tonkin AM, Shaw JE. Continuous relationships between non-diabetic hyperglycaemia and both cardiovascular disease and all-cause mortality: the Australian Diabetes, Obesity, and Lifestyle (AusDiab) study. Diabetologia 52: 415–424, 2009 - PubMed
-
- Beck LH. Changes in renal function with aging. Clin Geriatr Med 14: 199–209, 1998 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical