

Surgical site infections and other postoperative complications following prophylactic anticoagulation in total joint arthroplasty
- PMID: 24717837
- PMCID: PMC3981661
- DOI: 10.1371/journal.pone.0091755
Surgical site infections and other postoperative complications following prophylactic anticoagulation in total joint arthroplasty
Abstract
Background: Anticoagulants reduce the risk of venous thromboembolism (VTE) after total joint replacement. However, concern remains that pharmacologic VTE prophylaxis can lead to bleeding, which may impact on postoperative complications such as infections and reoperations.
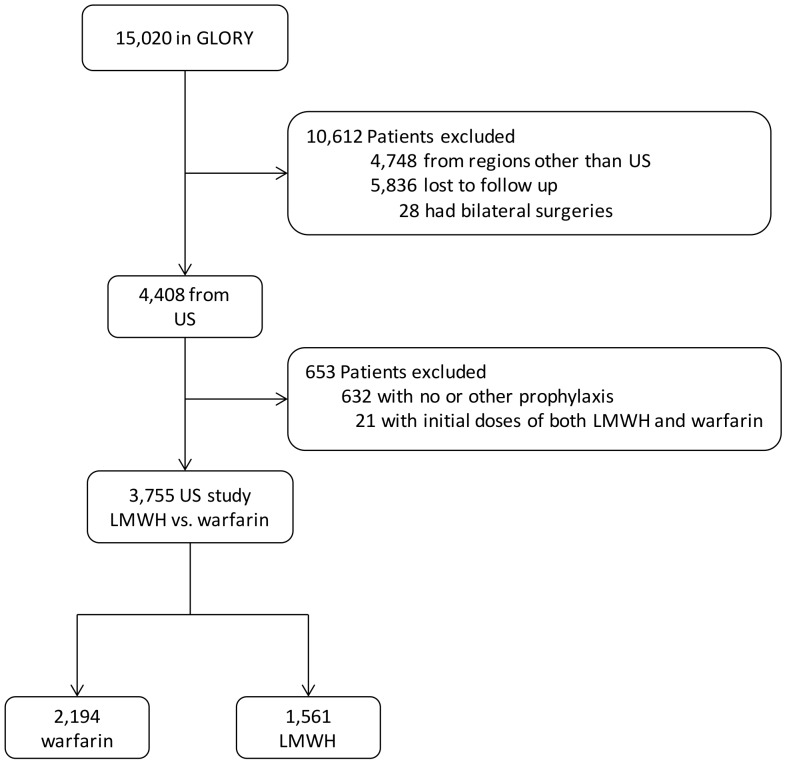
Methods and findings: From the Global Orthopedic Registry (GLORY), we reviewed 3,755 patients in US who elected for primary total hip or knee arthroplasty, received either warfarin or low molecular weight heparin (LMWH) as VTE prophylactics, and had up-to-90-day follow-up after discharge. We compared incidence rates of VTE, infections and other complications between LMWH and warfarin groups, and used multivariate analyses with propensity score weighting to generate the odds ratio (OR). Patients receiving LMWH tended to be older and higher in the American Society of Anesthesiologists grade scores. In contrast, warfarin was used more frequently for hip arthroplasty with longer duration among patients with more pre-existing comorbidity (all P<0.02). A weight variable was created with propensity score to account for differences in covariate distributions. Propensity score-weighted analyses showed no differences in VTE complications. However, compared to warfarin, LMWH was associated with significantly higher rates of bleeding (6.2% vs. 2.1%; OR = 3.82, 95% confidence interval [CI], 2.64 to 5.52), blood transfusion (29.4% vs. 22.0%; OR = 1.75, 95% CI, 1.51 to 2.04), reoperations (2.4% vs. 1.3%; OR = 1.77, 95% CI, 1.07 to 2.93) and infections (1.6% vs. 0.6%; OR = 2.79, 95% CI, 1.42 to 5.45). Similar results were obtained from compliant uses of warfarin (26%) and LMWH (62%) according to clinical guidelines. While surgical site infections were mostly superficial, current study was underpowered to compare incidence rates of deep infections (<1.0%).
Conclusions: Surgical site infections and reoperations in 3 months following primary total joint arthroplasty may be associated with anticoagulant use that exhibited higher bleeding risk. Long-term complications and deep wound infections remain to be studied.
Conflict of interest statement
Figures
References
-
- Falck-Ytter Y, Francis CW, Johanson NA, Curley C, Dahl OE, et al. (2012) Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 141: e278S–325S. - PMC - PubMed
-
- American Academy of Orthopedic Surgeons (2012) Guideline on Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty. http://www.aaos.org/research/guidelines/VTE/VTE_guideline.asp Accessed 25 January 2013
-
- Lieberman JR, Hsu WK (2005) Prevention of venous thromboembolic disease after total hip and knee arthroplasty. J Bone Joint Surg Am 87: 2097–2112. - PubMed
-
- Urquhart DM, Hanna FS, Brennan SL, Wluka AE, Leder K, et al. (2010) Incidence and risk factors for deep surgical site infection after primary total hip arthroplasty: a systematic review. J Arthroplasty 25: 1216–1222 e1211–1213. - PubMed
-
- Kurtz SM, Lau E, Schmier J, Ong KL, Zhao K, et al. (2008) Infection burden for hip and knee arthroplasty in the United States. J Arthroplasty 23: 984–991. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
