

Targeting mTOR dependency in pancreatic cancer
- PMID: 24717934
- PMCID: PMC4145424
- DOI: 10.1136/gutjnl-2013-306202
Targeting mTOR dependency in pancreatic cancer
Abstract
Objective: Pancreatic cancer is a leading cause of cancer-related death in the Western world. Current chemotherapy regimens have modest survival benefit. Thus, novel, effective therapies are required for treatment of this disease.
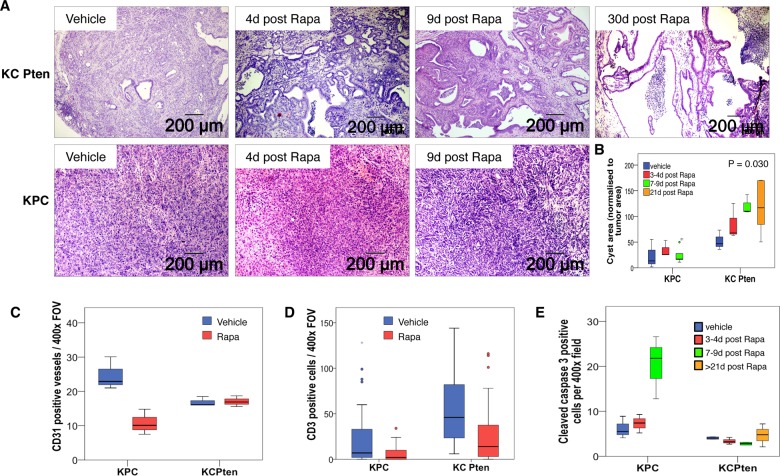
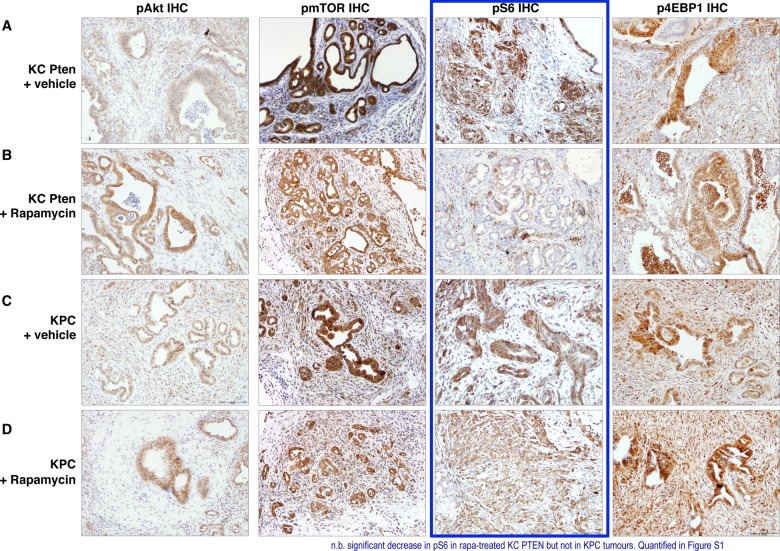
Design: Activating KRAS mutation almost always drives pancreatic tumour initiation, however, deregulation of other potentially druggable pathways promotes tumour progression. PTEN loss leads to acceleration of Kras(G12D)-driven pancreatic ductal adenocarcinoma (PDAC) in mice and these tumours have high levels of mammalian target of rapamycin (mTOR) signalling. To test whether these KRAS PTEN pancreatic tumours show mTOR dependence, we compared response to mTOR inhibition in this model, to the response in another established model of pancreatic cancer, KRAS P53. We also assessed whether there was a subset of pancreatic cancer patients who may respond to mTOR inhibition.
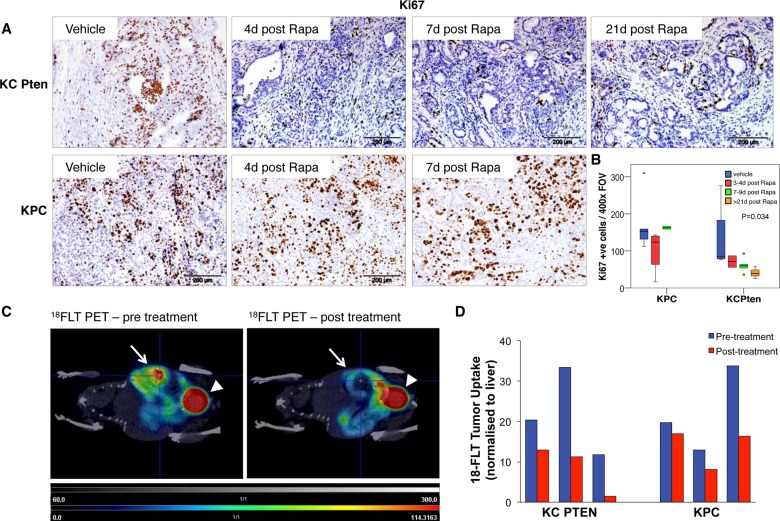
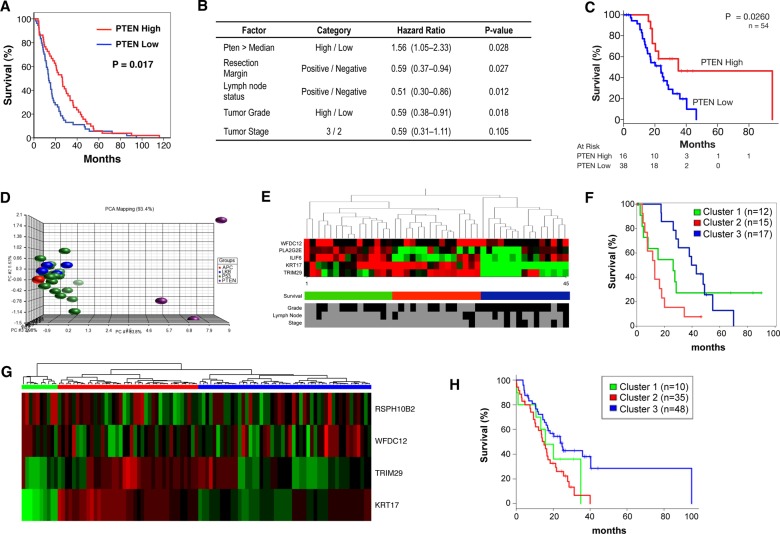
Results: We found that tumours in KRAS PTEN mice exhibit a remarkable dependence on mTOR signalling. In these tumours, mTOR inhibition leads to proliferative arrest and even tumour regression. Further, we could measure response using clinically applicable positron emission tomography imaging. Importantly, pancreatic tumours driven by activated KRAS and mutant p53 did not respond to treatment. In human tumours, approximately 20% of cases demonstrated low PTEN expression and a gene expression signature that overlaps with murine KRAS PTEN tumours.
Conclusions: KRAS PTEN tumours are uniquely responsive to mTOR inhibition. Targeted anti-mTOR therapies may offer clinical benefit in subsets of human PDAC selected based on genotype, that are dependent on mTOR signalling. Thus, the genetic signatures of human tumours could be used to direct pancreatic cancer treatment in the future.
Keywords: Cell Signalling; Genetics; Pancreatic Cancer; Pharmacogenomics.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures

Comment in
-
Use of a preclinical model of pancreas cancer to identify potential candidates for rapalogue therapy.Gut. 2014 Sep;63(9):1379-80. doi: 10.1136/gutjnl-2014-307317. Epub 2014 Jun 25. Gut. 2014. PMID: 24966285 No abstract available.
References
-
- Burris HA, III, Moore MJ, Andersen J, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 1997;15:2403–13 - PubMed
-
- Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011;364:1817–25 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous