

Preoperative factors affecting length of stay after elective anterior cervical discectomy and fusion with and without corpectomy: a multivariate analysis of an academic center cohort
- PMID: 24718069
- PMCID: PMC4024365
- DOI: 10.1097/BRS.0000000000000307
Preoperative factors affecting length of stay after elective anterior cervical discectomy and fusion with and without corpectomy: a multivariate analysis of an academic center cohort
Abstract
Study design: Retrospective cohort study of 183 patients who underwent elective anterior cervical discectomy and fusion (ACDF) at a single institution during a 2-year period.
Objective: To determine which preoperative factors were independently associated with a prolonged hospital length of stay (LOS) after ACDF.
Summary of background data: ACDF has become the most common treatment modality for addressing cervical spine pathology. Extended LOS after ACDF is associated with increased costs and complications. There is a lack of conclusive data for factors affecting LOS after ACDF. This study aims to create a multivariate model to determine the association of various patient and operative characteristics with LOS after ACDF.
Methods: Patients who underwent elective ACDF at a single academic institution between January 2011 and February 2013 were identified using billing records. Their charts were reviewed to collect variables available preoperatively such as patient demographics, comorbidities, and surgery planned. Patients were categorized as normal or extended LOS, with extended LOS defined as LOS more than the 75th percentile. A multivariate logistic regression was used to determine which factors were independently associated with extended LOS.
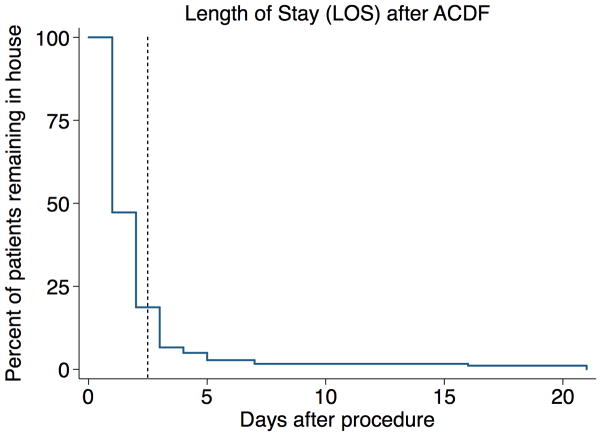
Results: A total of 183 patients with ACDF were identified. The average LOS for this cohort was 2.0 ± 2.5 days (mean ± standard deviation). Extended LOS was defined as 3 days or more. Multivariate analysis revealed that preoperative factors independently associated with extended LOS were history of nonspinal malignancy (odds ratio [OR] = 4.9), history of pulmonary disease (OR = 4.0), and procedures that included corpectomy (OR = 4.5).
Conclusion: Patients with a history of nonspinal malignancy or pulmonary disease, as well as patients who underwent corpectomy, were more likely to have an extended LOS (ORs, 4.0-4.9). Of significant note, other factors that one might expect to be associated with extended LOS did not independently predict extended LOS in this analysis.
Level of evidence: 3.
Figures
References
-
- Yue WM, Brodner W, Highland TR. Long-term results after anterior cervical discectomy and fusion with allograft and plating: a 5- to 11-year radiologic and clinical follow-up study. Spine. 2005;30:2138–44. - PubMed
-
- Klein GR, Vaccaro AR, Albert TJ. Health outcome assessment before and after anterior cervical discectomy and fusion for radiculopathy: a prospective analysis. Spine. 2000;25:801–3. - PubMed
-
- Gephart MG, Zygourakis CC, Arrigo RT, et al. Venous thromboembolism after thoracic/thoracolumbar spinal fusion. World neurosurgery. 2012;78:545–52. - PubMed
-
- Fineberg SJ, Nandyala SV, Marquez-Lara A, et al. Incidence and risk factors for postoperative delirium after lumbar spine surgery. Spine. 2013;38:1790–6. - PubMed
-
- Epstein NE, Schwall G, Reillly T, et al. Surgeon choices, and the choice of surgeons, affect total hospital charges for single-level anterior cervical surgery. Spine. 2011;36:905–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
