

Response of functional mitral regurgitation during dobutamine infusion in relation to changes in left ventricular dyssynchrony and mitral valve geometry
- PMID: 24719124
- PMCID: PMC3990066
- DOI: 10.3349/ymj.2014.55.3.592
Response of functional mitral regurgitation during dobutamine infusion in relation to changes in left ventricular dyssynchrony and mitral valve geometry
Abstract
Purpose: Functional mitral regurgitation (FMR) and myocardial dyssynchrony commonly occur in patients with dilated cardiomyopathy (DCM). The aim of this study was to elucidate changes in FMR in relation to those in left ventricular (LV) dyssynchrony as well as geometric parameters of the mitral valve (MV) in DCM patients during dobutamine infusion.
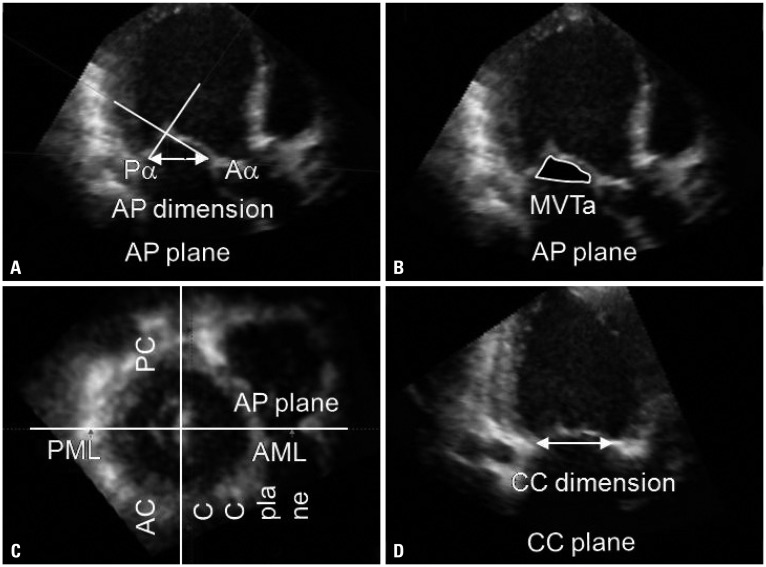
Materials and methods: Twenty-nine DCM patients (M:F=15:14; age: 62±15 yrs) with FMR underwent echocardiography at baseline and during peak dose (30 or 40 ug/min) of dobutamine infusion. Using 2D echocardiography, LV end-diastolic volume, end-systolic volume (LVESV), ejection fraction (EF), and effective regurgitant orifice area (ERO) were estimated. Dyssynchrony indices (DIs), defined as the standard deviation of time interval-to-peak myocardial systolic contraction of eight LV segments, were measured. Using the multi-planar reconstructive mode from commercially available 3D image analysis software, MV tenting area (MVTa) was measured. All geometrical measurements were corrected (c) by the height of each patient.
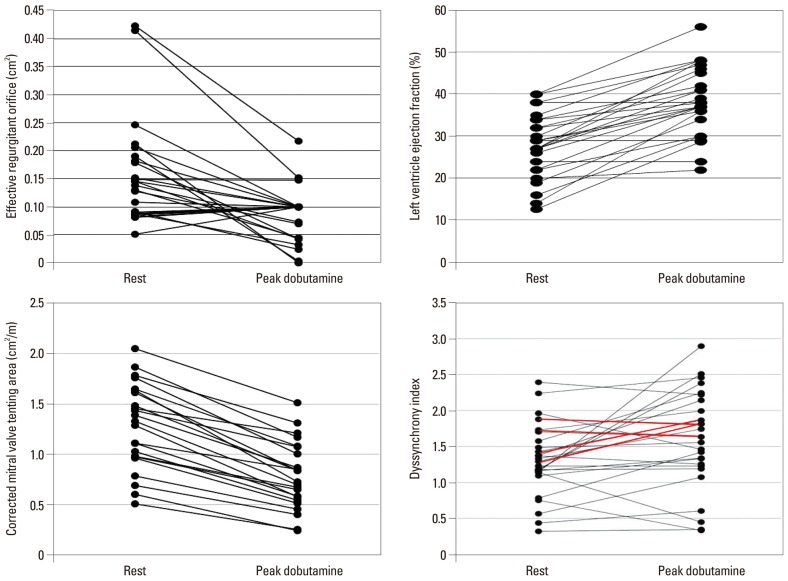
Results: During dobutamine infusion, EF (28±8% vs. 39±11%, p=0.001) improved along with significant decrease in cLVESV (80.1±35.2 mm³/m vs. 60.4±31.1 mm³/m, p=0.001); cMVTa (1.28±0.48 cm²/m vs. 0.79±0.33 cm²/m, p=0.001) was significantly reduced; and DI (1.31±0.51 vs. 1.58±0.68, p=0.025) showed significant increase. Despite significant deterioration of LV dyssynchrony during dobutamine infusion, ERO (0.16±0.09 cm² vs. 0.09±0.08 cm², p=0.001) significantly improved. On multivariate analysis, ΔcMVTa and ΔEF were found to be the strongest independent determinants of ΔERO (R²=0.443, p=0.001).
Conclusion: Rather than LV dyssynchrony, MV geometry determined by LV geometry and systolic pressure, which represents the MV closing force, may be the primary determinant of MR severity.
Keywords: Mitral regurgitation; dobutamine; dyssynchrony.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
Similar articles
-
Role of dyssynchrony on functional mitral regurgitation in patients with idiopathic dilated cardiomyopathy: a comparison study with geometric parameters of mitral apparatus.J Cardiovasc Ultrasound. 2011 Jun;19(2):69-75. doi: 10.4250/jcu.2011.19.2.69. Epub 2011 Jun 30. J Cardiovasc Ultrasound. 2011. PMID: 21860720 Free PMC article.
-
Role of regional mechanical dyssynchrony as a determinant of functional mitral regurgitation in patients with left ventricular systolic dysfunction.Heart. 2006 Oct;92(10):1390-5. doi: 10.1136/hrt.2005.082115. Epub 2006 Jan 31. Heart. 2006. PMID: 16449509 Free PMC article.
-
Dobutamine-induced improvement in inferior myocardial contractile function predicts reduction in functional mitral regurgitation: a study using tissue Doppler strain rate imaging.Circ Cardiovasc Imaging. 2010 Nov;3(6):638-46. doi: 10.1161/CIRCIMAGING.110.937300. Epub 2010 Sep 8. Circ Cardiovasc Imaging. 2010. PMID: 20826593
-
Mechanical dyssynchrony and functional mitral regurgitation: pathophysiology and clinical implications.J Cardiovasc Med (Hagerstown). 2008 May;9(5):461-9. doi: 10.2459/JCM.0b013e3282ef39c5. J Cardiovasc Med (Hagerstown). 2008. PMID: 18403997 Review.
-
Proportionate and Disproportionate Functional Mitral Regurgitation: A New Conceptual Framework That Reconciles the Results of the MITRA-FR and COAPT Trials.JACC Cardiovasc Imaging. 2019 Feb;12(2):353-362. doi: 10.1016/j.jcmg.2018.11.006. Epub 2018 Dec 12. JACC Cardiovasc Imaging. 2019. PMID: 30553663 Review.
References
-
- Blondheim DS, Jacobs LE, Kotler MN, Costacurta GA, Parry WR. Dilated cardiomyopathy with mitral regurgitation: decreased survival despite a low frequency of left ventricular thrombus. Am Heart J. 1991;122(3 Pt 1):763–771. - PubMed
-
- Tahta SA, Oury JH, Maxwell JM, Hiro SP, Duran CM. Outcome after mitral valve repair for functional ischemic mitral regurgitation. J Heart Valve Dis. 2002;11:11–18. - PubMed
-
- Tomita T, Nakatani S, Eishi K, Takemura T, Takasawa A, Koyanagi H, et al. [Effectiveness of surgical repair of mitral regurgitation concomitant with dilated cardiomyopathy] J Cardiol. 1998;32:391–396. - PubMed
-
- Otsuji Y, Handschumacher MD, Schwammenthal E, Jiang L, Song JK, Guerrero JL, et al. Insights from three-dimensional echocardiography into the mechanism of functional mitral regurgitation: direct in vivo demonstration of altered leaflet tethering geometry. Circulation. 1997;96:1999–2008. - PubMed
-
- Otsuji Y, Handschumacher MD, Liel-Cohen N, Tanabe H, Jiang L, Schwammenthal E, et al. Mechanism of ischemic mitral regurgitation with segmental left ventricular dysfunction: three-dimensional echocardiographic studies in models of acute and chronic progressive regurgitation. J Am Coll Cardiol. 2001;37:641–648. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
