

Finding the 'ideal' regimen for fentanyl-based intravenous patient-controlled analgesia: how to give and what to mix?
- PMID: 24719151
- PMCID: PMC3990071
- DOI: 10.3349/ymj.2014.55.3.800
Finding the 'ideal' regimen for fentanyl-based intravenous patient-controlled analgesia: how to give and what to mix?
Abstract
Purpose: This analysis was done to investigate the optimal regimen for fentanyl-based intravenous patient-controlled analgesia (IV-PCA) by finding a safe and effective background infusion rate and assessing the effect of adding adjuvant drugs to the PCA regimen.
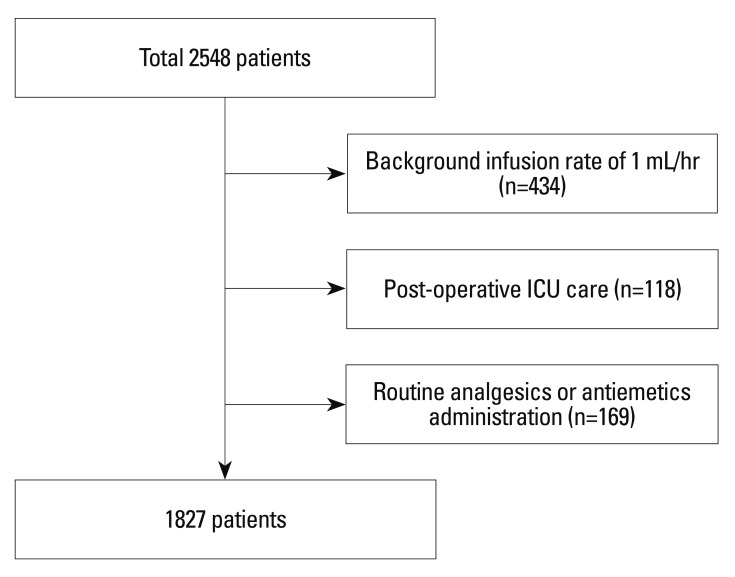
Materials and methods: Background infusion rate of fentanyl, type of adjuvant analgesic and/or antiemetic that was added to the IV-PCA, and patients that required rescue analgesics and/or antiemetics were retrospectively reviewed in 1827 patients who underwent laparoscopic abdominal surgery at a single tertiary hospital.
Results: Upon multivariate analysis, lower background infusion rates, younger age, and IV-PCA without adjuvant analgesics were identified as independent risk factors of rescue analgesic administration. Higher background infusion rates, female gender, and IV-PCA without additional 5HT₃ receptor blockers were identified as risk factors of rescue antiemetics administration. A background infusion rate of 0.38 μg/kg/hr [area under the curve (AUC) 0.638] or lower required rescue analgesics in general, whereas, addition of adjuvant analgesics decreased the rate to 0.37 μg/kg/hr (AUC 0.712) or lower. A background infusion rate of 0.36 μg/kg/hr (AUC 0.638) or higher was found to require rescue antiemetics in general, whereas, mixing antiemetics with IV-PCA increased the rate to 0.37 μg/kg/hr (AUC 0.651) or higher.
Conclusion: Background infusion rates of fentanyl between 0.12 and 0.67 μg/kg/hr may safely be used without any serious side effects for IV-PCA. In order to approach the most reasonable background infusion rate for effective analgesia without increasing postoperative nausea and vomiting, adding an adjuvant analgesic and an antiemetic should always be considered.
Keywords: Analgesia; adjuvant drug; background infusion rate; fentanyl; patient-controlled.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Palmer PP, Miller RD. Current and developing methods of patient-controlled analgesia. Anesthesiol Clin. 2010;28:587–599. - PubMed
-
- Ballantyne JC, Carr DB, Chalmers TC, Dear KB, Angelillo IF, Mosteller F. Postoperative patient-controlled analgesia: meta-analyses of initial randomized control trials. J Clin Anesth. 1993;5:182–193. - PubMed
-
- Walder B, Schafer M, Henzi I, Tramèr MR. Efficacy and safety of patient-controlled opioid analgesia for acute postoperative pain. A quantitative systematic review. Acta Anaesthesiol Scand. 2001;45:795–804. - PubMed
-
- Momeni M, Crucitti M, De Kock M. Patient-controlled analgesia in the management of postoperative pain. Drugs. 2006;66:2321–2337. - PubMed
-
- Kim SH, Shin YS, Oh YJ, Lee JR, Chung SC, Choi YS. Risk assessment of postoperative nausea and vomiting in the intravenous patient-controlled analgesia environment: predictive values of the Apfel's simplified risk score for identification of high-risk patients. Yonsei Med J. 2013;54:1273–1281. - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
