

Criteria for preserving posterior cruciate ligament depending on intra-operative gap measurement in total knee replacement
- PMID: 24719296
- PMCID: PMC3985198
- DOI: 10.1302/2046-3758.34.2000228
Criteria for preserving posterior cruciate ligament depending on intra-operative gap measurement in total knee replacement
Abstract
Objectives: Because posterior cruciate ligament (PCL) resection makes flexion gaps wider in total knee replacement (TKR), preserving or sacrificing a PCL affects the gap equivalence; however, there are no criteria for the PCL resection that consider gap situations of each knee. This study aims to investigate gap characteristics of knees and to consider the criteria for PCL resection.
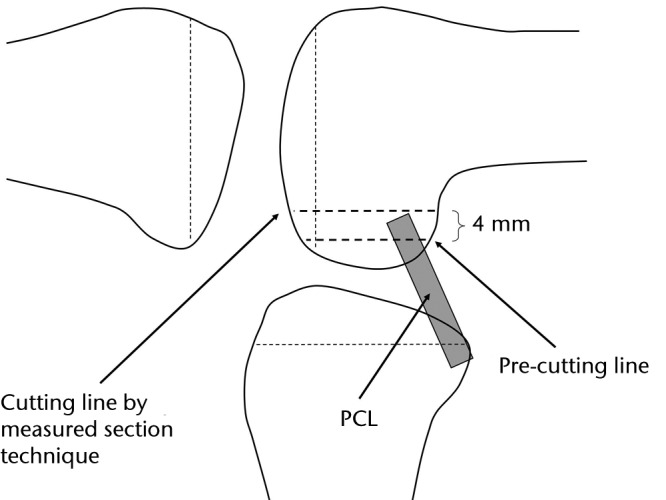
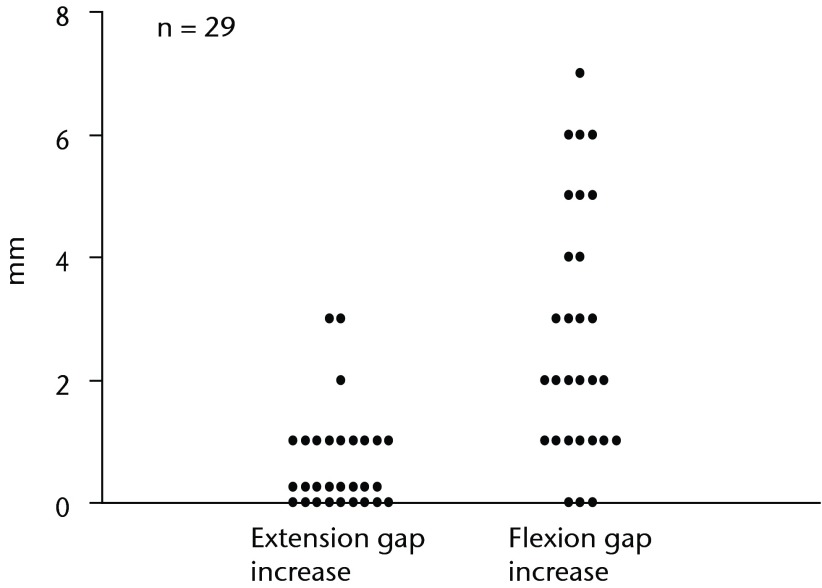
Methods: The extension and flexion gaps were measured, first with the PCL preserved and subsequently with the PCL removed (in cases in which posterior substitute components were selected). The PCL preservation or sacrifice was solely determined by the gap measurement results, without considering other functions of the PCL such as 'roll back.'
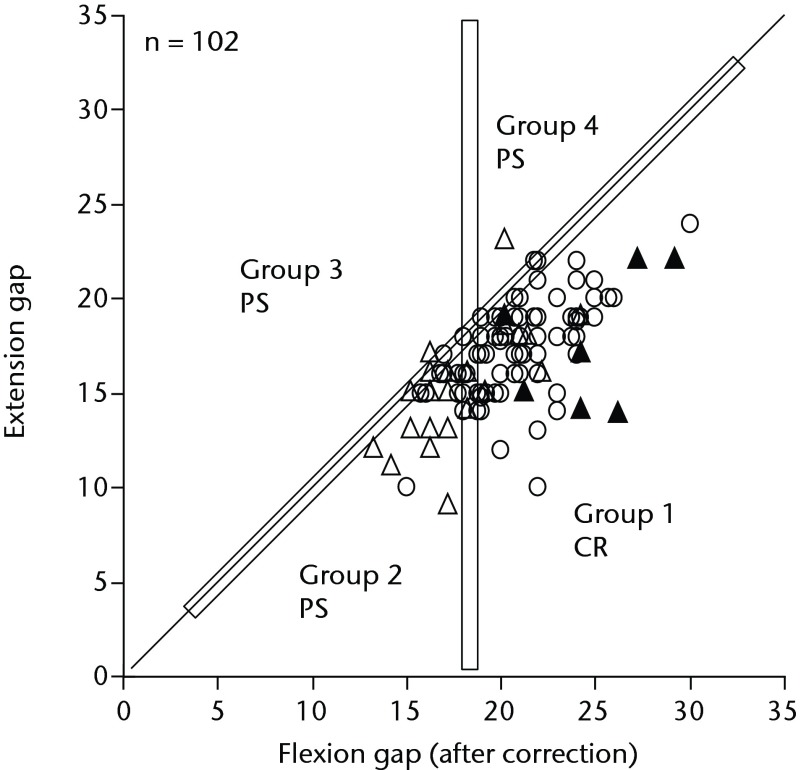
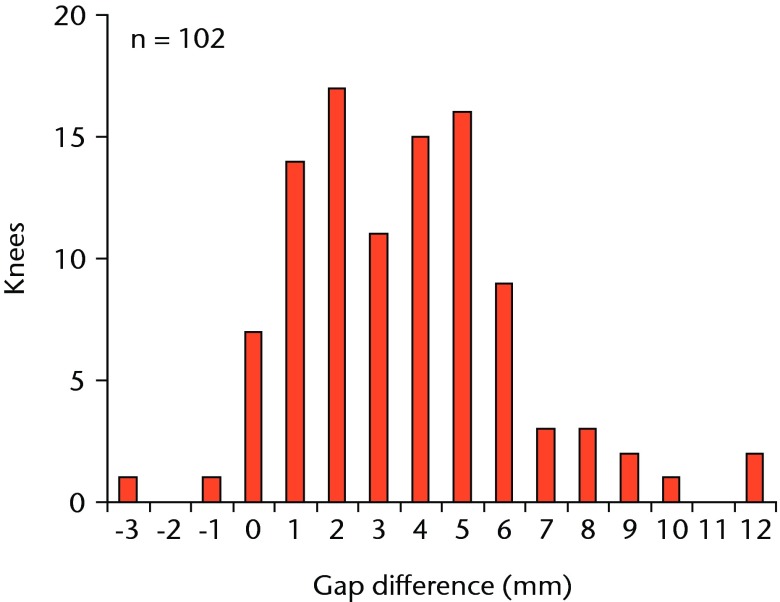
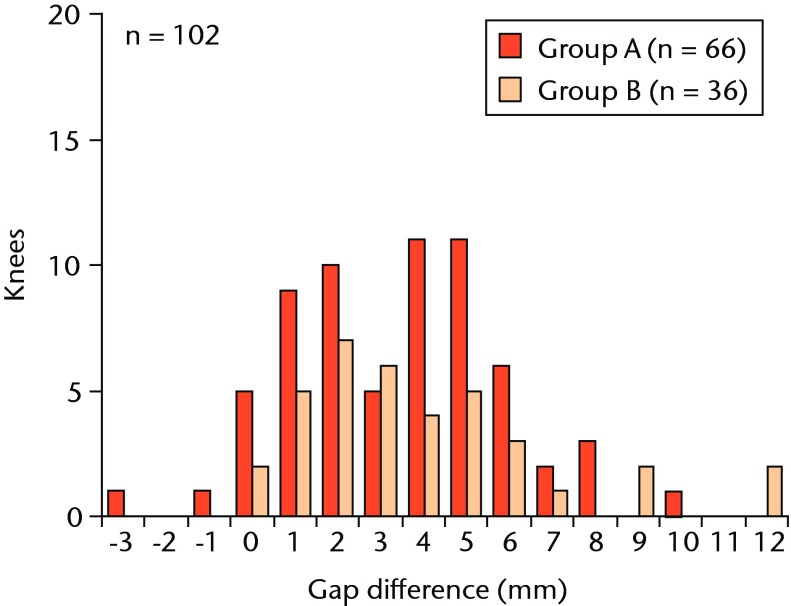
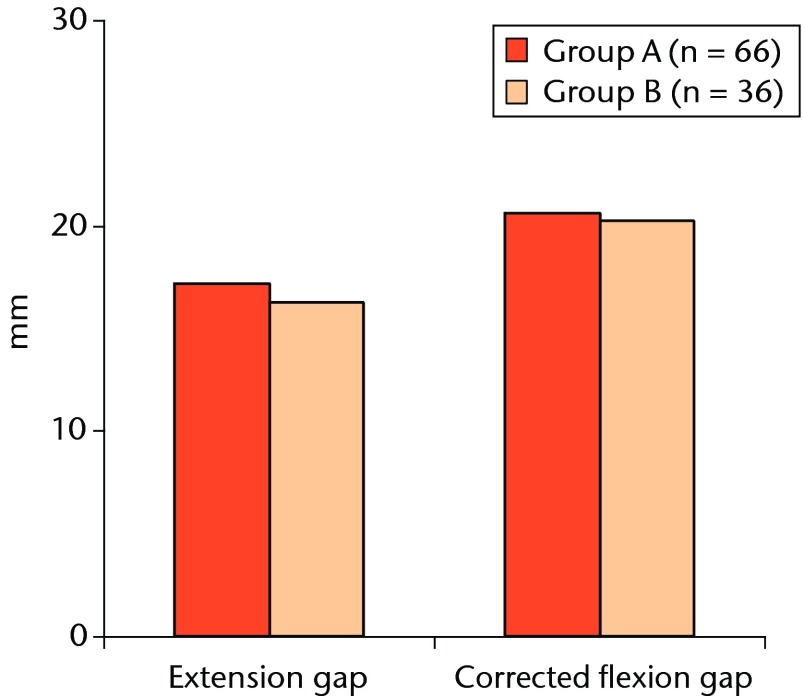
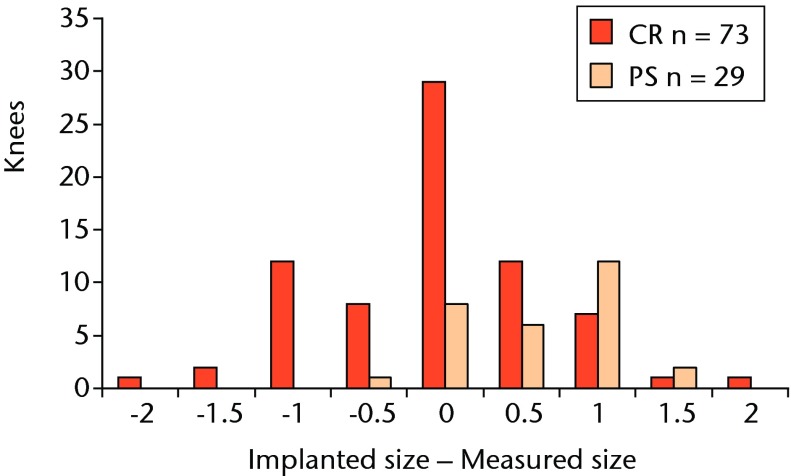
Results: Wide variations were observed in the extension and flexion gaps. The flexion gaps were significantly larger than the extension gaps. Cases with 18 mm or more flexion gap and with larger flexion than extension gap were implanted with cruciate retaining component. A posterior substitute component was implanted with the other cases.
Conclusions: In order to make adequate gaps, it is important to decide whether to preserve the PCL based on the intra-operative gap measurements made with the PCL intact. Cite this article: Bone Joint Res 2014;3:95-100.
Keywords: Arthroplasty; Gap; Knee; Posterior cruciate ligament.
Conflict of interest statement
Figures

Similar articles
-
Posterior cruciate ligament resection in total knee arthroplasty: the effect on flexion-extension gaps, mediolateral laxity, and fixed flexion deformity.Bone Joint J. 2019 Oct;101-B(10):1230-1237. doi: 10.1302/0301-620X.101B10.BJJ-2018-1428.R2. Bone Joint J. 2019. PMID: 31564152
-
Comparative evaluation of posterior cruciate ligament in total knee arthroplasty.J Orthop Surg (Hong Kong). 2017 Jan;25(1):2309499017690976. doi: 10.1177/2309499017690976. J Orthop Surg (Hong Kong). 2017. PMID: 28219307
-
The Role of Complete Posterior Cruciate Ligament Release in Flexion Gap Balancing for Total Knee Arthroplasty.J Arthroplasty. 2019 Jul;34(7S):S361-S365. doi: 10.1016/j.arth.2019.03.017. Epub 2019 Mar 13. J Arthroplasty. 2019. PMID: 30948290
-
Posterior cruciate ligament-retaining, posterior stabilized, and varus/valgus posterior stabilized constrained articulations in total knee arthroplasty.Instr Course Lect. 2006;55:419-27. Instr Course Lect. 2006. PMID: 16958477 Review.
-
[Combined posterior and anterior cruciate ligament reconstruction : Arthroscopic treatment with the GraftLink® system].Oper Orthop Traumatol. 2019 Feb;31(1):20-35. doi: 10.1007/s00064-018-0580-6. Epub 2018 Dec 18. Oper Orthop Traumatol. 2019. PMID: 30564843 Review. German.
Cited by
-
Large flexion contracture angle predicts tight extension gap during navigational posterior stabilized-type total knee arthroplasty with the pre-cut technique: a retrospective study.BMC Musculoskelet Disord. 2022 Jan 22;23(1):78. doi: 10.1186/s12891-022-05035-z. BMC Musculoskelet Disord. 2022. PMID: 35065647 Free PMC article.
-
Preoperative Factors Predicting the Preservation of the Posterior Cruciate Ligament in Total Knee Arthroplasty.Orthop Surg. 2022 Sep;14(9):2203-2209. doi: 10.1111/os.13439. Epub 2022 Aug 17. Orthop Surg. 2022. PMID: 35979544 Free PMC article.
-
Three-year clinical and radiological results of a cruciate-retaining type of the knee prosthesis with anatomical geometry developed in Japan.BMC Musculoskelet Disord. 2021 Mar 3;22(1):241. doi: 10.1186/s12891-021-04114-x. BMC Musculoskelet Disord. 2021. PMID: 33658001 Free PMC article.
-
Intraoperative factors affecting conversion from cruciate retaining to cruciate substituting in total knee arthroplasty.Knee Surg Sports Traumatol Arthrosc. 2016 Oct;24(10):3247-3253. doi: 10.1007/s00167-015-3971-3. Epub 2016 Jan 5. Knee Surg Sports Traumatol Arthrosc. 2016. PMID: 26733275
References
-
- Colizza WA, Insall JN, Scuderi GR. The posterior stabilized total knee prosthesis: assessment of polyethylene damage and osteolysis after a 10 year minimum follow-up. J Bone Joint Surg [Am] 1995;77-A:1713–1720 - PubMed
-
- Migakaka KC, Ranawat C, Mullaji A. 10 to 20 years follow-up of total knee arthroplasty for valgus deformities. Clin Orthop Relat Res 1997;345:29–37 - PubMed
-
- Ritter MA, Herbst SA, Keating EM, Faris PM, Meding JB. Long-term survival analysis of a posterior cruciate-retaining total condylar total knee arthroplasty. Clin Orthop Relat Res 1994;309:136–145 - PubMed
-
- Tanzer M, Smith K, Burnett S. Posterior-stabilized versus cruciate-retaining total knee arthroplasty. Balancing the gap. J Arthroplasty 2002;17:813–819 - PubMed
-
- Rand JA, Trousdale RT, Ilstrup DM, Harmsen WS. Factors affecting the durability of primary total knee prostheses. J Bone Joint Surg [Am] 2003;85-A:259–265 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
