

Application of ultrasonic bone curette in endoscopic endonasal skull base surgery: technical note
- PMID: 24719795
- PMCID: PMC3969437
- DOI: 10.1055/s-0033-1354580
Application of ultrasonic bone curette in endoscopic endonasal skull base surgery: technical note
Abstract
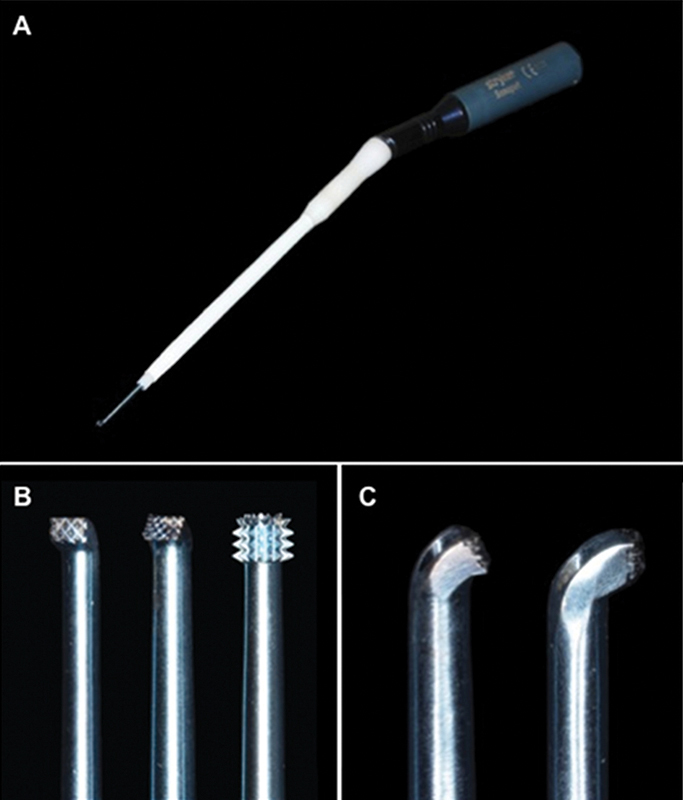
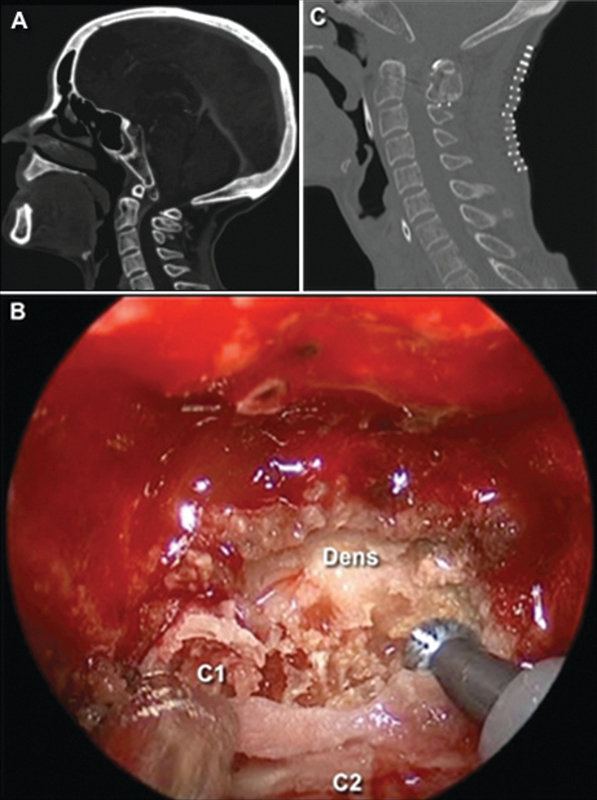
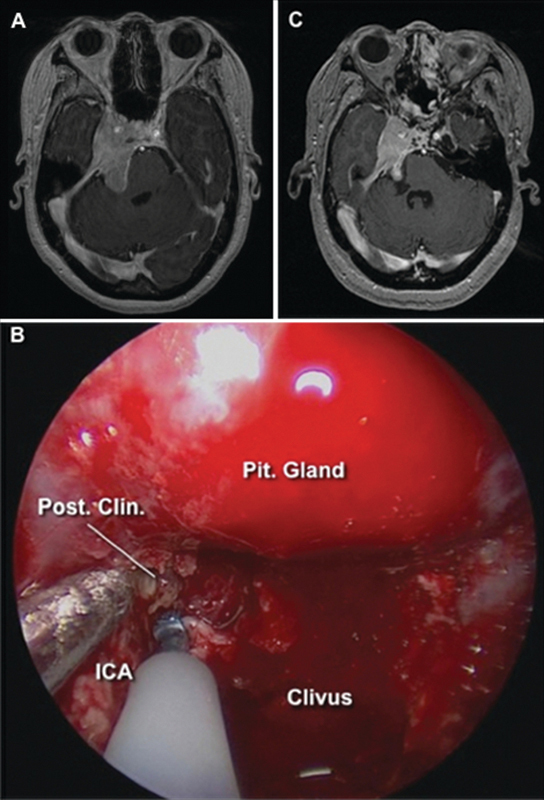
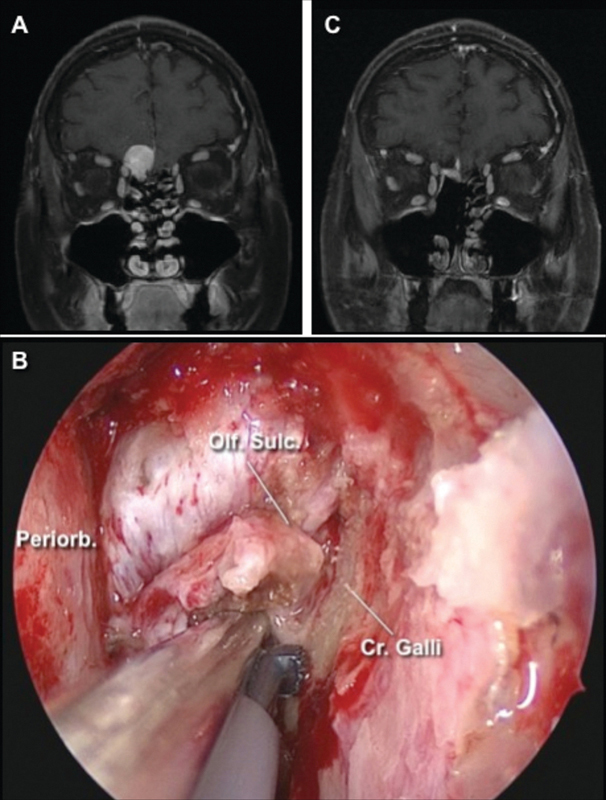
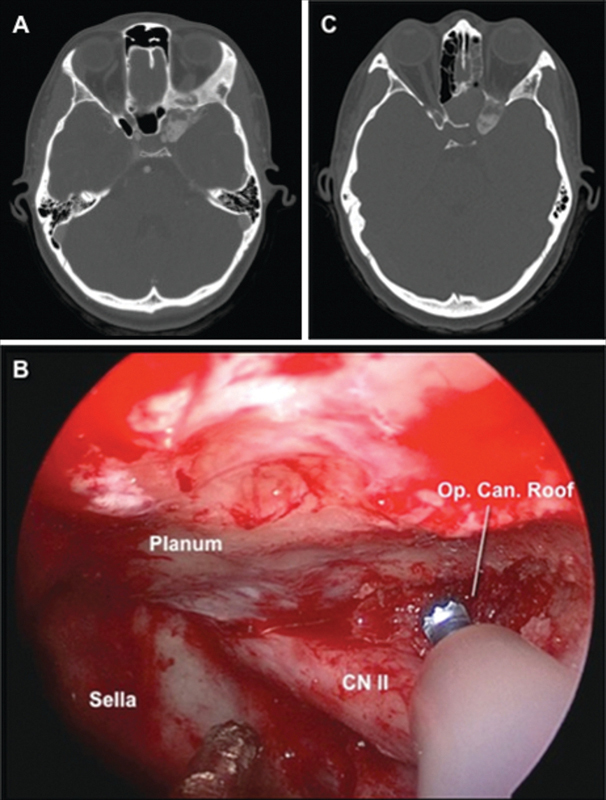
Background Endoscopic endonasal surgery (EES) of the skull base often requires extensive bone work in proximity to critical neurovascular structures. Objective To demonstrate the application of an ultrasonic bone curette during EES. Methods Ten patients with skull base lesions underwent EES from September 2011 to April 2012 at the University of Pittsburgh Medical Center. Most of the bone work was done with high-speed drill and rongeurs. The ultrasonic curette was used to remove specific structures. Results All the patients were submitted to fully endoscopic endonasal procedures and had critical bony structures removed with the ultrasonic bone curette. Two patients with degenerative spine diseases underwent odontoid process removal. Five patients with clival and petroclival tumors underwent posterior clinoid removal. Two patients with anterior fossa tumors underwent crista galli removal. One patient underwent unilateral optic nerve decompression. No mechanical or heat injury resulted from the ultrasonic curette. The surrounding neurovascular structures and soft tissue were preserved in all cases. Conclusion In selected EES, the ultrasonic bone curette was successfully used to remove loose pieces of bone in narrow corridors, adjacent to neurovascular structures, and it has advantages to high-speed drills in these specific situations.
Keywords: bone removal; endoscopic endonasal; skull base; ultrasonic bone curette.
Figures
References
-
- Maroon J C. Skull base surgery: past, present, and future trends. Neurosurg Focus. 2005;19(1):E1. - PubMed
-
- Prevedello D M, Doglietto F, Jane J A Jr, Jagannathan J, Han J, Laws E R Jr. History of endoscopic skull base surgery: its evolution and current reality. J Neurosurg. 2007;107(1):206–213. - PubMed
-
- Snyderman C H, Pant H, Carrau R L, Prevedello D, Gardner P, Kassam A B. What are the limits of endoscopic sinus surgery?: the expanded endonasal approach to the skull base. Keio J Med. 2009;58(3):152–160. - PubMed
-
- Yamasaki T, Moritake K, Nagai H, Uemura T, Shingu T, Matsumoto Y. A new, miniature ultrasonic surgical aspirator with a handpiece designed for transsphenoidal surgery. Technical note. J Neurosurg. 2003;99(1):177–179. - PubMed
-
- Pagella F, Giourgos G, Matti E, Colombo A, Carena P. Removal of a fronto-ethmoidal osteoma using the Sonopet omni ultrasonic bone curette: first impressions. Laryngoscope. 2008;118(2):307–309. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
