

Possible extracardiac predictors of aortic dissection in Marfan syndrome
- PMID: 24720641
- PMCID: PMC4021409
- DOI: 10.1186/1471-2261-14-47
Possible extracardiac predictors of aortic dissection in Marfan syndrome
Abstract
Background: According to previous studies, aortic diameter alone seems to be insufficient to predict the event of aortic dissection in Marfan syndrome (MFS). Determining the optimal schedule for preventive aortic root replacement (ARR) aortic growth rate is of importance, as well as family history, however, none of them appear to be decisive. Thus, the aim of this study was to search for potential predictors of aortic dissection in MFS.
Methods: A Marfan Biobank consisting of 79 MFS patients was established. Thirty-nine MFS patients who underwent ARR were assigned into three groups based on the indication for surgery (dissection, annuloaortic ectasia and prophylactic surgery). The prophylactic surgery group was excluded from the study. Transforming growth factor-β (TGF-β) serum levels were measured by ELISA, relative expression of c-Fos, matrix metalloproteinase 3 and 9 (MMP-3 and -9) were assessed by RT-PCR. Clinical parameters, including anthropometric variables - based on the original Ghent criteria were also analyzed.
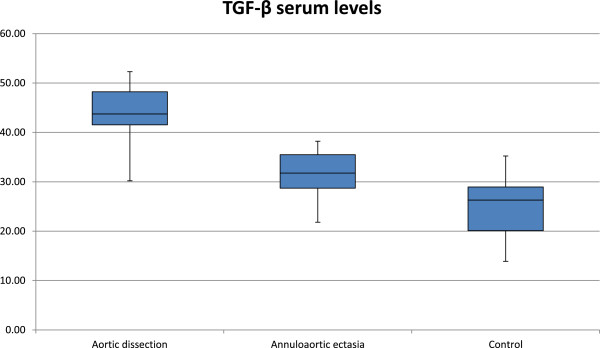
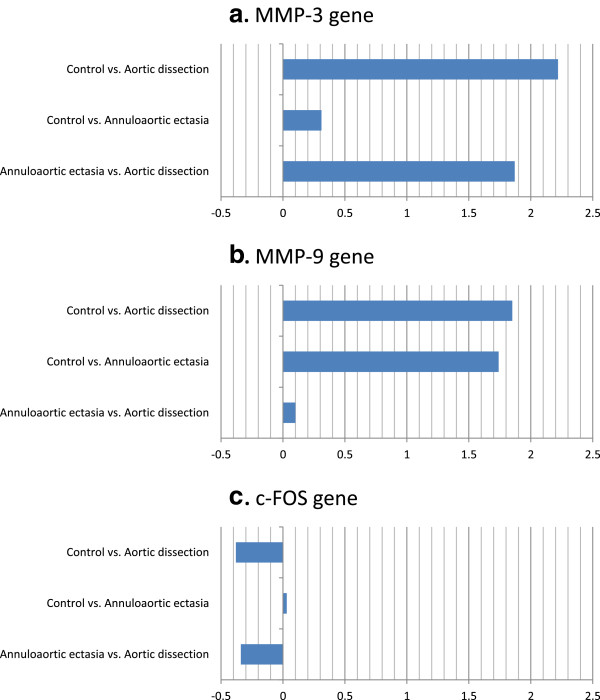
Results: Among patients with aortic dissection, TGF-β serum level was elevated (43.78 ± 6.51 vs. 31.64 ± 4.99 ng/l, p < 0.0001), MMP-3 was up-regulated (Ln2α = 1.87, p = 0.062) and striae atrophicae were more common (92% vs. 41% p = 0.027) compared to the annuloaortic ectasia group.
Conclusions: We found three easily measurable parameters (striae atrophicae, TGF-β serum level, MMP-3) that may help to predict the risk of aortic dissection in MFS. Based on these findings a new classification of MFS, that is benign or malignant is also proposed, which could be taken into consideration in determining the timing of prophylactic ARR.
Figures
References
-
- Holm TM, Habashi JP, Doyle JJ, Bedja D, Chen Y, van Erp C, Lindsay ME, Kim D, Schoenhoff F, Cohn RD, Loeys BL, Thomas CJ, Patnaik S, Marugan JJ, Judge DP, Dietz HC. Noncanonical TGFβ signaling contributes to aortic aneurysm progression in Marfan syndrome mice. Science. 2011;332(6027):358–361. doi: 10.1126/science.1192149. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
