

Left ventricular amyloid deposition in patients with heart failure and preserved ejection fraction
- PMID: 24720917
- PMCID: PMC3984539
- DOI: 10.1016/j.jchf.2013.11.004
Left ventricular amyloid deposition in patients with heart failure and preserved ejection fraction
Abstract
Objectives: This study sought to determine the frequency of left ventricular amyloid in heart failure with preserved ejection fraction (HFpEF).
Background: Left ventricular amyloid deposition can cause diastolic dysfunction and HFpEF.
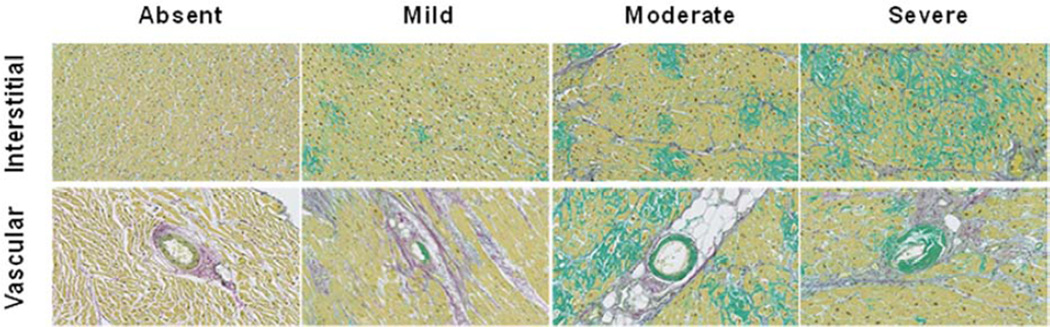
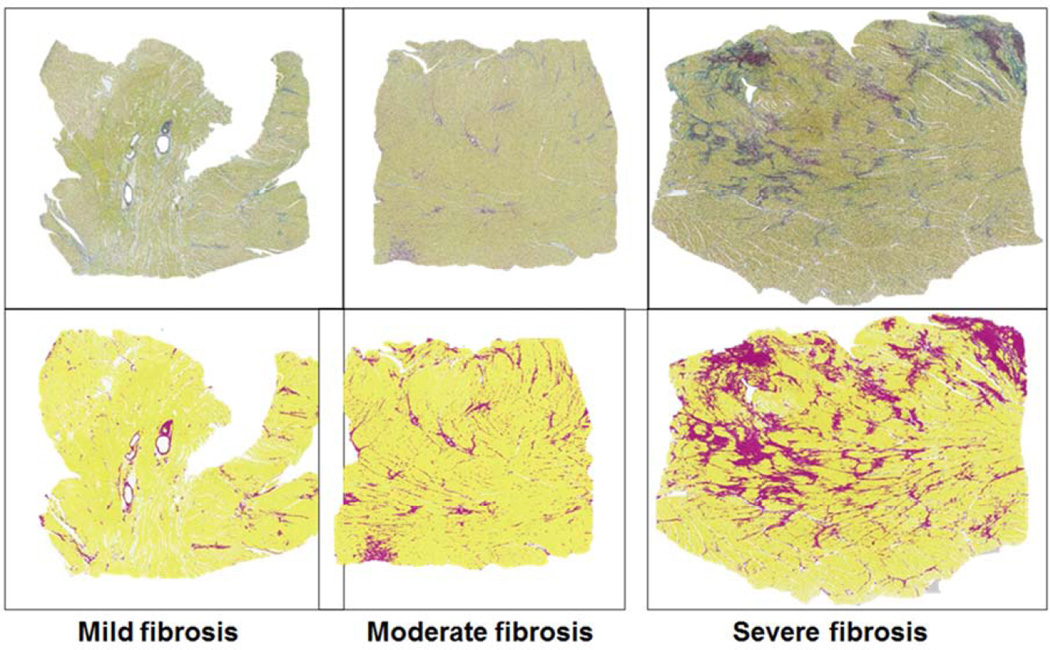
Methods: Autopsy of left ventricular specimens from patients with antemortem diagnosis of HFpEF without clinically apparent amyloid (n = 109) and from control subjects (n = 131) were screened with sulfated Alcian blue and subsequent Congo red staining with microdissection for mass spectrometry-based proteomics to determine amyloid type. Fibrosis was assessed with quantitative whole-field digital microscopy.
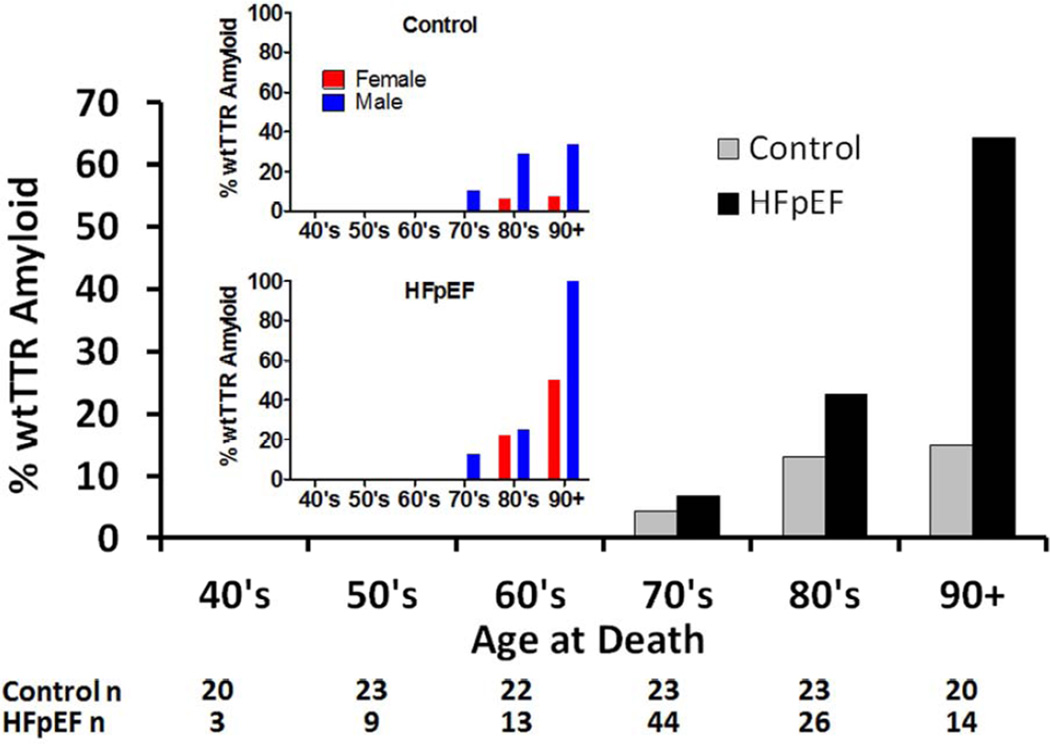
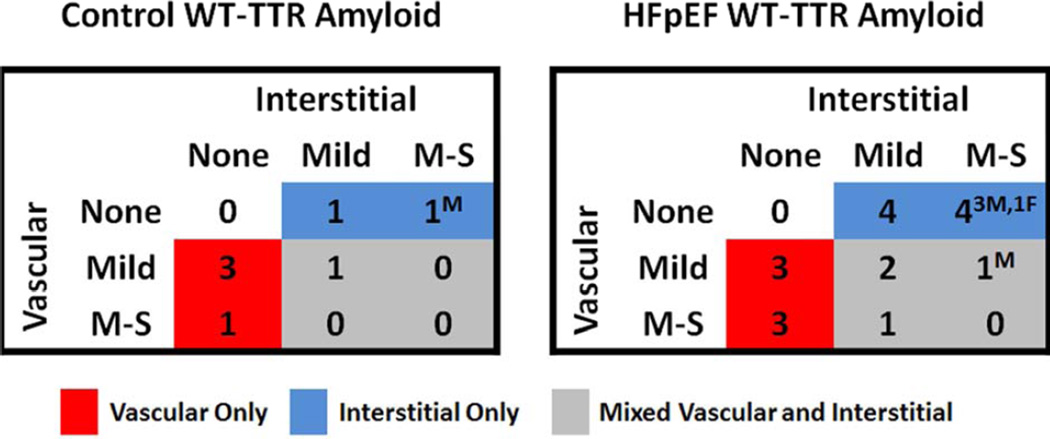
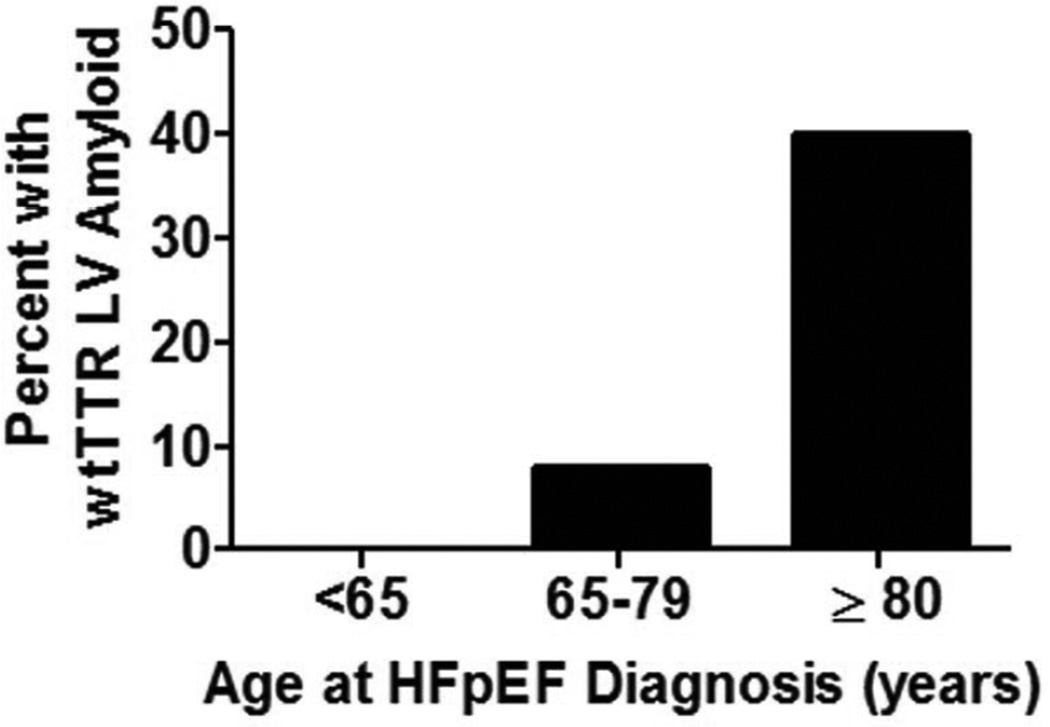
Results: The presence of wild-type transthyretin (wtTTR) amyloid was associated with age at death and male sex, but the age- and sex-adjusted prevalence of wtTTR amyloid was higher in HFpEF patients than in control subjects (odds ratio: 3.8, 95% confidence interval: 1.5 to 11.3; p = 0.03). Among HFpEF patients, moderate or severe interstitial wtTTR deposition, consistent with senile systemic amyloidosis as the primary etiology of HFpEF, was present in 5 (5%) patients (80% men), with mild interstitial and/or variable severity of intramural coronary vascular deposition in 13 (12%) patients. While, wtTTR deposition was often mild, adjusting for age and presence of HFpEF, wtTTR amyloid was associated with more fibrosis (p = 0.005) and lower age, sex, and body size-adjusted heart weight (p = 0.04).
Conclusions: Given the age- and sex-independent association of HFpEF and wtTTR deposition and an emerging understanding of the pathophysiology of the amyloidoses, the current findings support further investigation of the role of wtTTR in the pathophysiology of HFpEF.
Keywords: aging; amyloid; autopsy; diastole; heart failure with preserved ejection fraction; mass spectrometry-based proteomics; transthyretin.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Cornwell GG, 3rd, Murdoch WL, Kyle RA, Westermark P, Pitkanen P. Frequency and distribution of senile cardiovascular amyloid. A clinicopathologic correlation. Am J Med. 1983;75:618–623. - PubMed
-
- Tanskanen M, Peuralinna T, Polvikoski T, et al. Senile systemic amyloidosis affects 25% of the very aged and associates with genetic variation in alpha2-macroglobulin and tau: a population-based autopsy study. Ann Med. 2008;40:232–239. - PubMed
-
- Buerger L, Braunstein H. Senile cardiac amyloidosis. Am J Med. 1960;28:357–367. - PubMed
-
- Hodkinson HM, Pomerance A. The clinical significance of senile cardiac amyloidosis: a prospective clinico-pathological study. Q J Med. 1977;46:381–387. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UL1 TR000135/TR/NCATS NIH HHS/United States
- TL1 TR000137/TR/NCATS NIH HHS/United States
- T32 HL007111/HL/NHLBI NIH HHS/United States
- R01 HL072435/HL/NHLBI NIH HHS/United States
- R01 HL105418/HL/NHLBI NIH HHS/United States
- U01 HL084907/HL/NHLBI NIH HHS/United States
- T32-HL07111/HL/NHLBI NIH HHS/United States
- U10 HL110262/HL/NHLBI NIH HHS/United States
- P01 HL076611/HL/NHLBI NIH HHS/United States
- R01 HL055502/HL/NHLBI NIH HHS/United States
- U01HL84907/HL/NHLBI NIH HHS/United States
- P01HL 76611/HL/NHLBI NIH HHS/United States
- HL 55502/HL/NHLBI NIH HHS/United States
- U01HL 84907/HL/NHLBI NIH HHS/United States
- HL 72435/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
