

Adherence to guideline-recommended therapy is associated with decreased major adverse cardiovascular events and major adverse limb events among patients with peripheral arterial disease
- PMID: 24721799
- PMCID: PMC4187469
- DOI: 10.1161/JAHA.113.000697
Adherence to guideline-recommended therapy is associated with decreased major adverse cardiovascular events and major adverse limb events among patients with peripheral arterial disease
Abstract
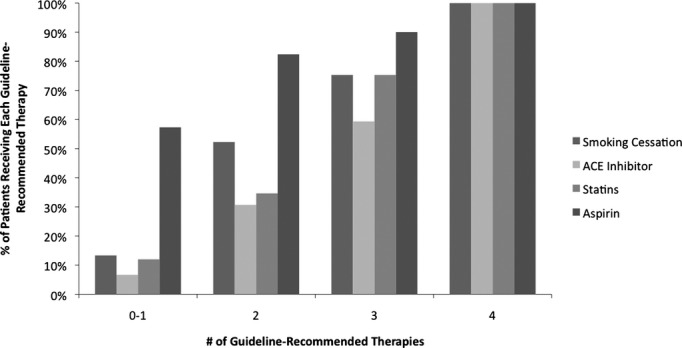
Background: Current guidelines recommend that patients with peripheral arterial disease (PAD) cease smoking and be treated with aspirin, statin medications, and angiotensin-converting enzyme (ACE) inhibitors. The combined effects of multiple guideline-recommended therapies in patients with symptomatic PAD have not been well characterized.
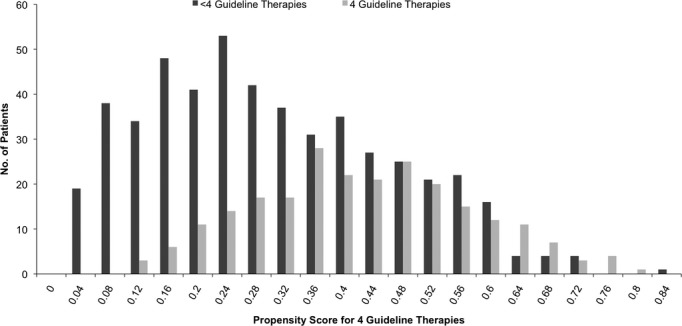
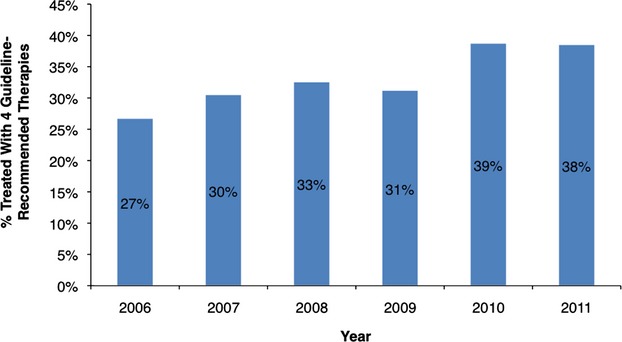
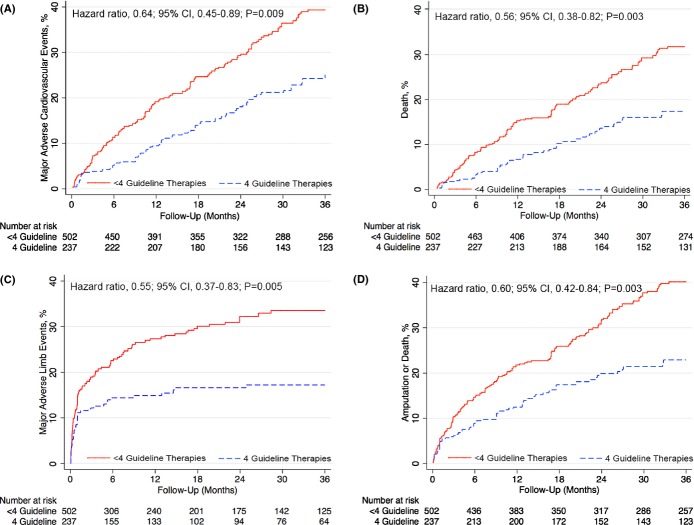
Methods and results: We analyzed a comprehensive database of all patients with claudication or critical limb ischemia (CLI) who underwent diagnostic or interventional lower-extremity angiography between June 1, 2006 and May 1, 2013 at a multidisciplinary vascular center. Baseline demographics, clinical data, and long-term outcomes were obtained. Inverse probability of treatment propensity weighting was used to determine the 3-year risk of major adverse cardiovascular or cerebrovascular events (MACE; myocardial infarction, stroke, or death) and major adverse limb events (MALE; major amputation, thrombolysis, or surgical bypass). Among 739 patients with PAD, 325 (44%) had claudication and 414 (56%) had CLI. Guideline-recommended therapies at baseline included use of aspirin in 651 (88%), statin medications in 496 (67%), ACE inhibitors in 445 (60%), and smoking abstention in 528 (71%) patients. A total of 237 (32%) patients met all four guideline-recommended therapies. After adjustment for baseline covariates, patients adhering to all four guideline-recommended therapies had decreased MACE (hazard ratio [HR], 0.64; 95% CI, 0.45 to 0.89; P=0.009), MALE (HR, 0.55; 95% CI, 0.37 to 0.83; P=0.005), and mortality (HR, 0.56; 95% CI, 0.38 to 0.82; P=0.003), compared to patients receiving less than four of the recommended therapies.
Conclusions: In patients with claudication or CLI, combination treatment with four guideline-recommended therapies is associated with significant reductions in MACE, MALE, and mortality.
Keywords: atherosclerosis; claudication; peripheral vascular disease; prevention; statins.
Figures
References
-
- Criqui MH, Fronek A, Barrett‐Connor E, Klauber MR, Gabriel S, Goodman D. The prevalence of peripheral arterial disease in a defined population. Circulation. 1985; 71:510-515 - PubMed
-
- Fowkes FG, Housley E, Cawood EH, Macintyre CC, Ruckley CV, Prescott RJ. Edinburgh Artery Study: prevalence of asymptomatic and symptomatic peripheral arterial disease in the general population. Int J Epidemiol. 1991; 20:384-392 - PubMed
-
- Meijer WT, Hoes AW, Rutgers D, Bots ML, Hofman A, Grobbee DE. Peripheral arterial disease in the elderly: the Rotterdam Study. Arterioscler Thromb Vasc Biol. 1998; 18:185-192 - PubMed
-
- Hirsch AT, Criqui MH, Treat‐Jacobson D, Regensteiner JG, Creager MA, Olin JW, Krook SH, Hunninghake DB, Comerota AJ, Walsh ME, McDermott MM, Hiatt WR. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA. 2001; 286:1317-1324 - PubMed
-
- Fowkes FGR, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, Norman PE, Sampson UK, Williams LJ, Mensah GA, Criqui MH. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013http://linkinghub.elsevier.com/retrieve/pii/S0140673613612490 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
