

National patterns of care and outcomes after combined modality therapy for stage IIIA non-small-cell lung cancer
- PMID: 24722151
- PMCID: PMC4274956
- DOI: 10.1097/JTO.0000000000000152
National patterns of care and outcomes after combined modality therapy for stage IIIA non-small-cell lung cancer
Abstract
Introduction: The role of surgery in addition to chemotherapy and radiation for stage IIIA non-small-cell lung cancer (NSCLC) remains controversial. Because there are limited data on the benefit from surgery in this setting, we evaluated the use of combined modality therapy nationally and explored the outcomes with and without the addition of surgery.
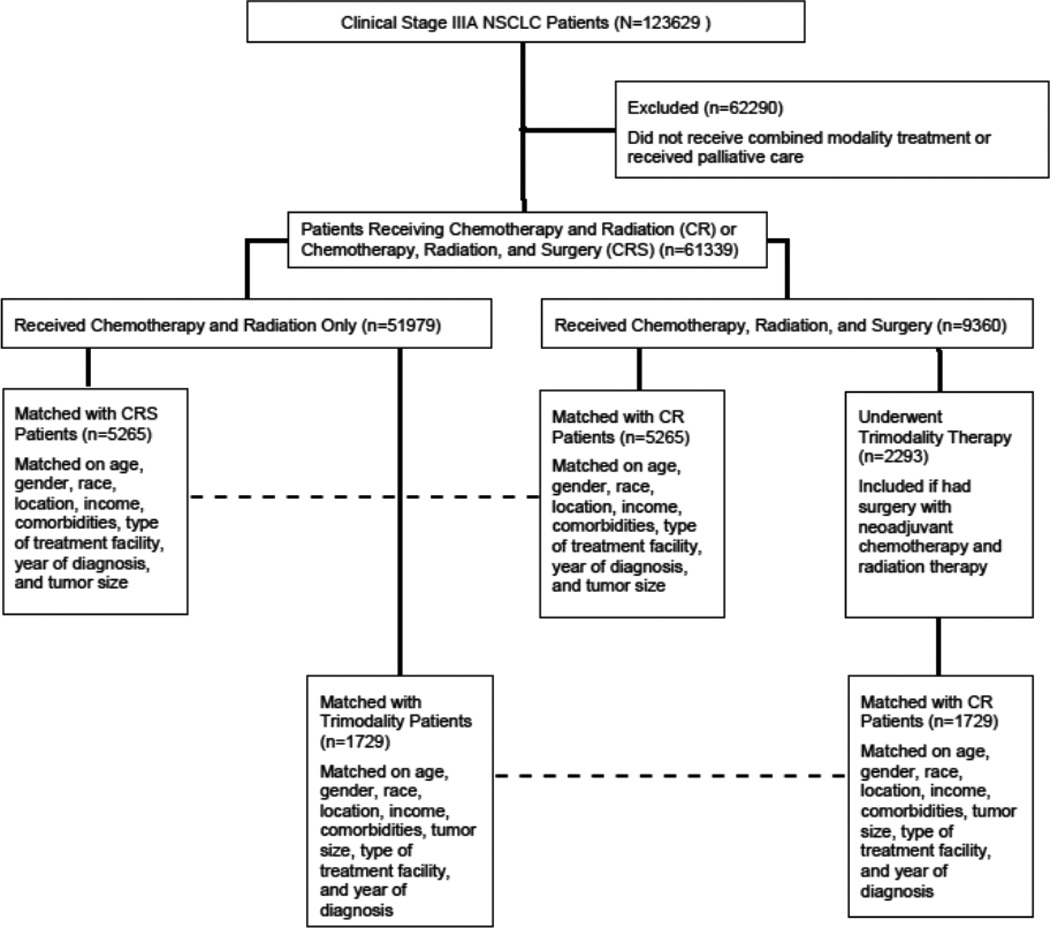
Methods: Patient variables and treatment-related outcomes were abstracted for patients with clinical stage IIIA NSCLC from the National Cancer Database. Patients receiving chemotherapy and radiation were compared with those undergoing chemotherapy, radiation, and surgery (CRS) in any sequence.
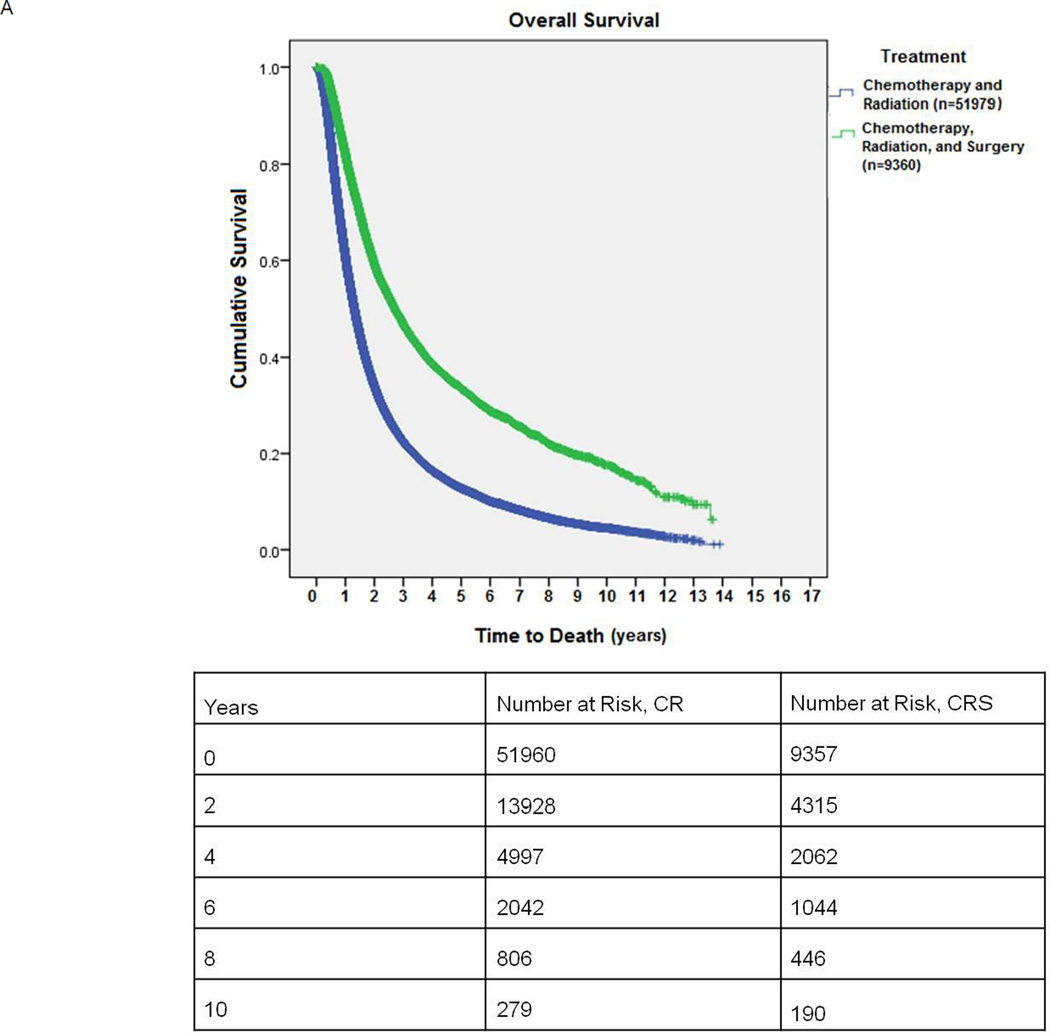
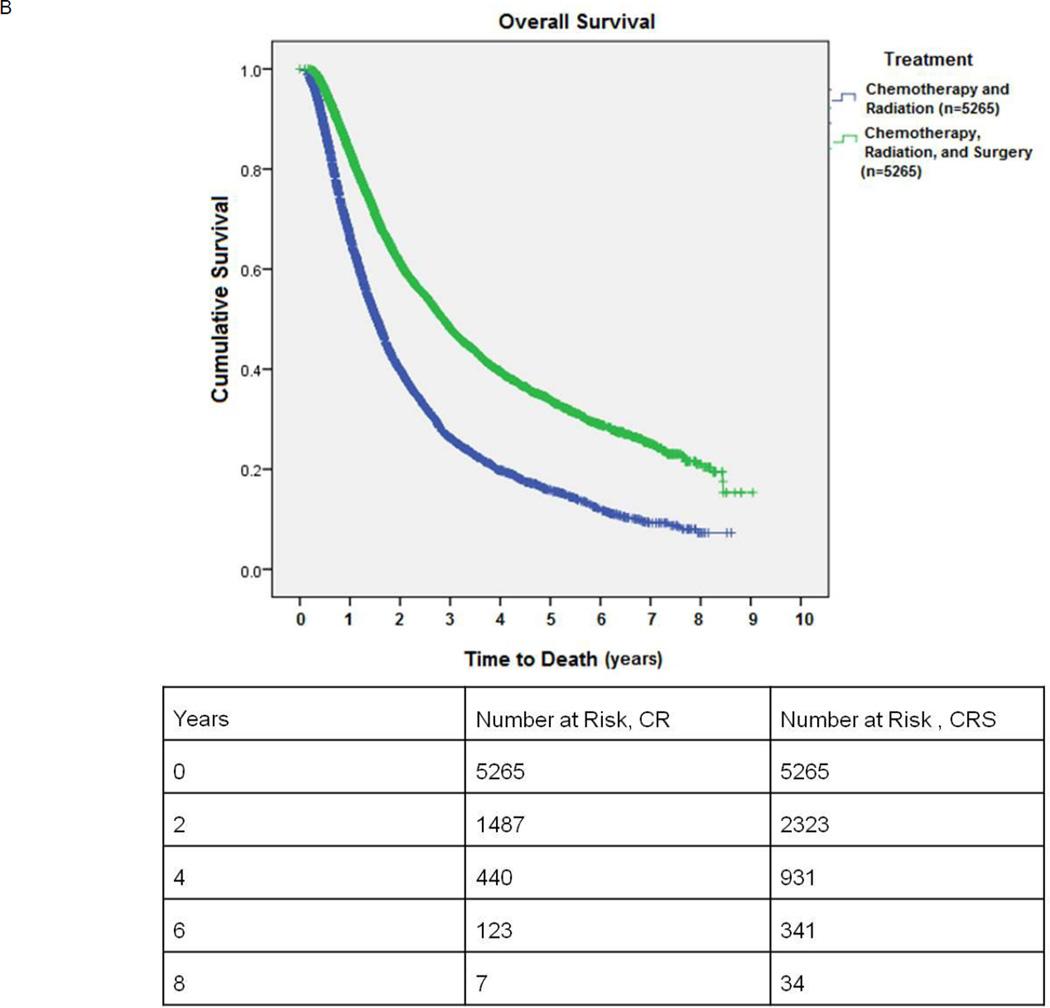
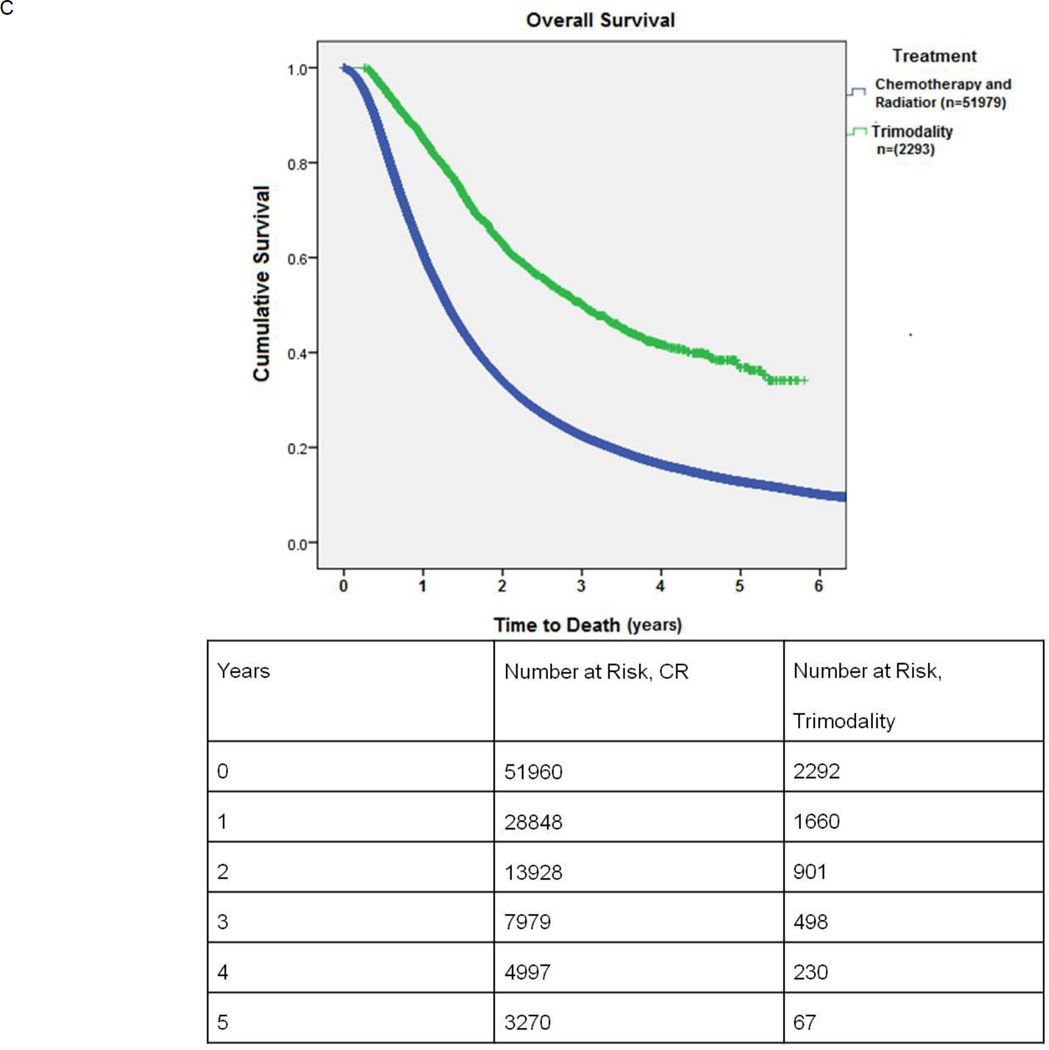
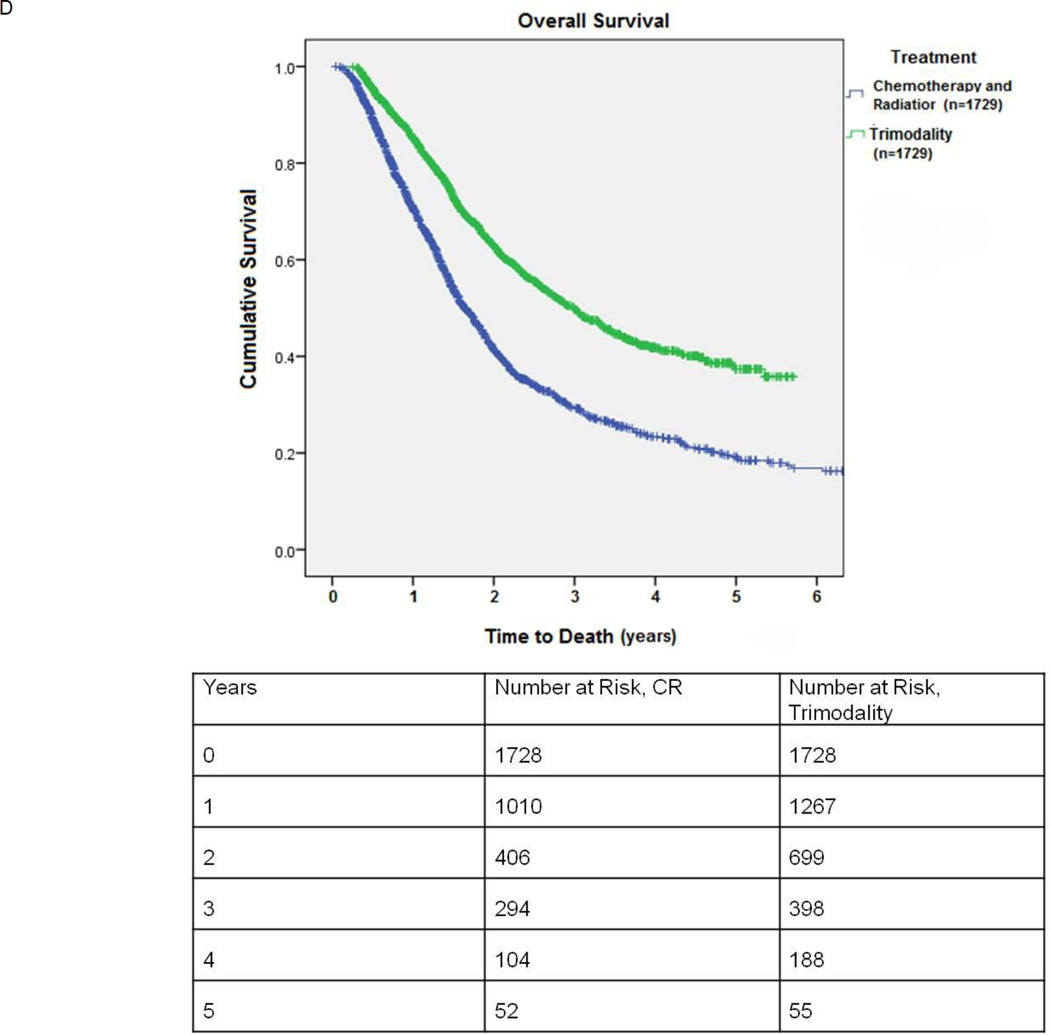
Results: Between 1998 and 2010, 61,339 patients underwent combined modality treatment for clinical stage IIIA NSCLC. Of these, 51,979 (84.7%) received chemotherapy and radiation while 9360 (15.3%) underwent CRS. Patients in the CRS group were younger, more likely female patients and Caucasians, and had smaller tumors and lower Charlson comorbidity scores. The 30-day surgical mortality was 200 of 8993 (2.2%). The median overall survival favored the CRS group in both unmatched (32.4 months versus 15.7 months, p < 0.001) and matched analysis based on patient characteristics (34.3 versus 18.4 months, p < 0.001).
Conclusions: There is significant heterogeneity in the treatment of stage IIIA NSCLC in the United States. Patients selected for surgery in addition to chemoradiation therapy seem to have better long-term survival.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Morgensztern D, Waqar S, Subramanian J, et al. Prognostic significance of tumor size in patients with stage III non-small-cell lung cancer: a surveillance, epidemiology, and end results (SEER) survey from 1998 to 2003. J Thorac Oncol. 2012;7:1479–1484. - PubMed
-
- Groome PA, Bolejack V, Crowley JJ, et al. The IASLC Lung Cancer Staging Project: validation of the proposals for revision of the T, N, and M descriptors and consequent stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol. 2007;2:694–705. - PubMed
-
- Salama JK, Vokes EE. New radiotherapy and chemoradiotherapy approaches for non-small-cell lung cancer. J Clin Oncol. 2013;31:1029–1038. - PubMed
-
- Bradley JD, Paulus R, Komaki R, et al. A randomized phase III comparison of standard-dose (60 Gy) versus high-dose (74 Gy) conformal chemoradiotherapy with or without cetuximab for stage III non-small cell lung cancer: Results on radiation dose in RTOG 0617. ASCO Meeting Abstracts. 2013;31:7501.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
