

Benchmarking outcomes in the critically injured burn patient
- PMID: 24722222
- PMCID: PMC4283803
- DOI: 10.1097/SLA.0000000000000438
Benchmarking outcomes in the critically injured burn patient
Abstract
Objective: To determine and compare outcomes with accepted benchmarks in burn care at 6 academic burn centers.
Background: Since the 1960s, US morbidity and mortality rates have declined tremendously for burn patients, likely related to improvements in surgical and critical care treatment. We describe the baseline patient characteristics and well-defined outcomes for major burn injuries.
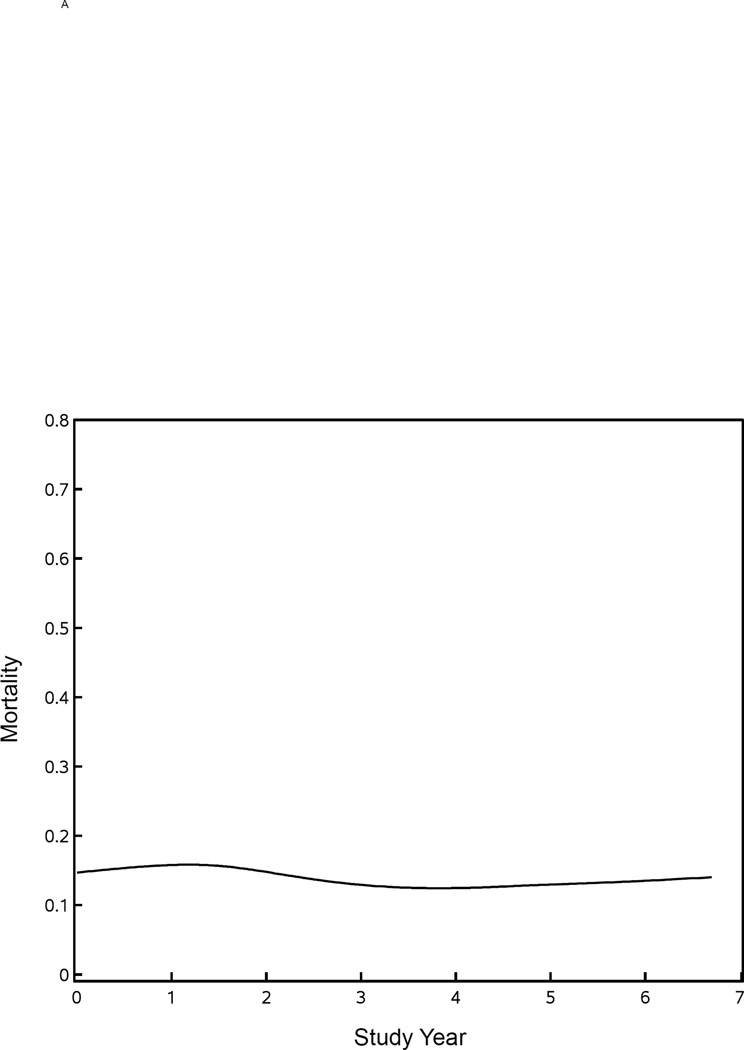
Methods: We followed 300 adults and 241 children from 2003 to 2009 through hospitalization, using standard operating procedures developed at study onset. We created an extensive database on patient and injury characteristics, anatomic and physiological derangement, clinical treatment, and outcomes. These data were compared with existing benchmarks in burn care.
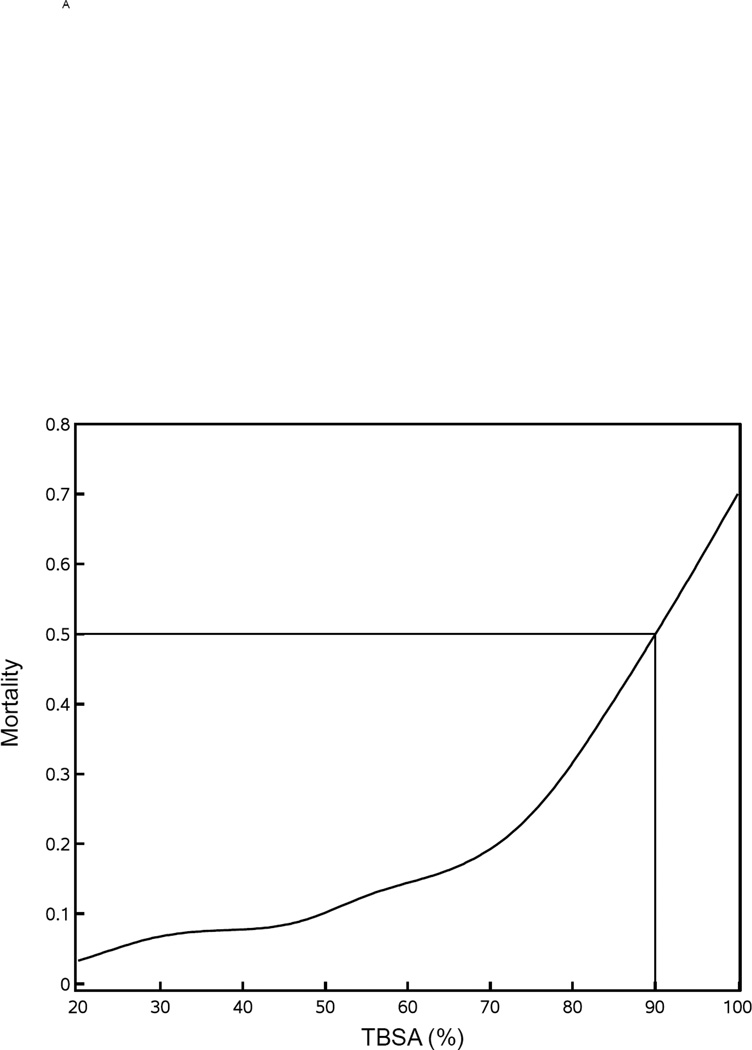
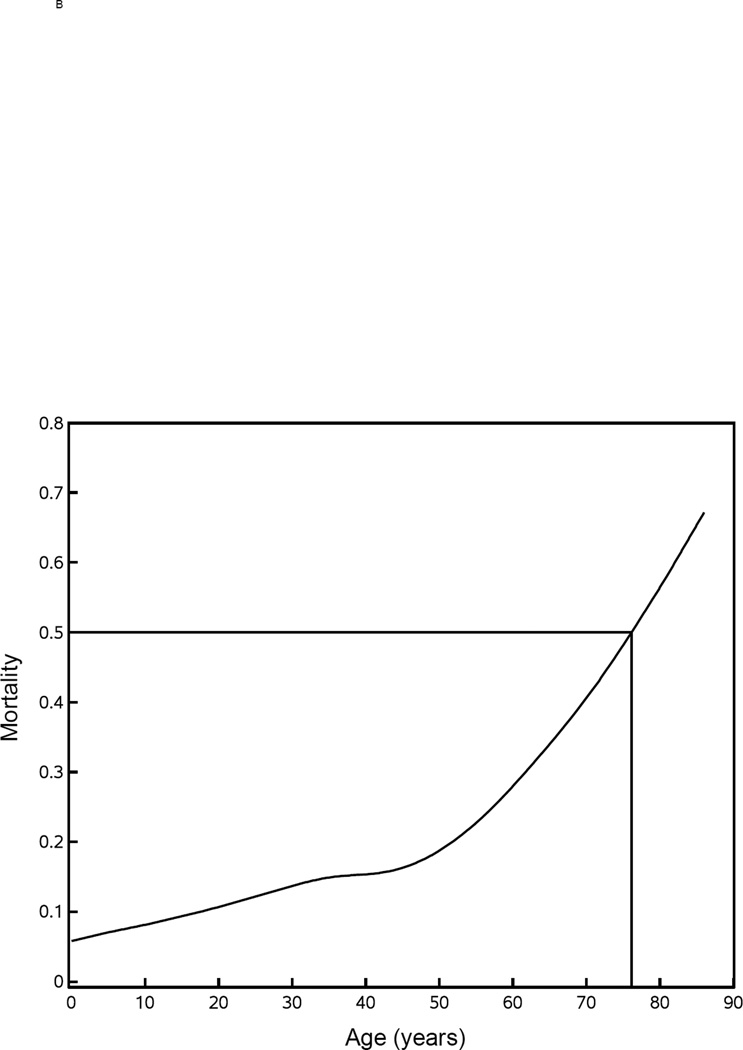
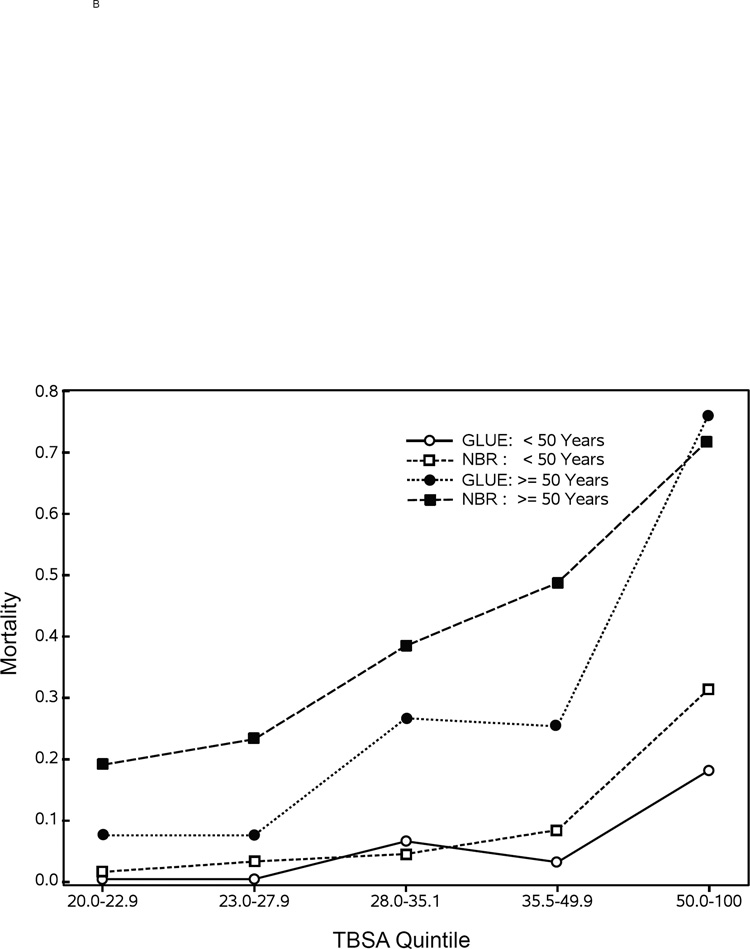
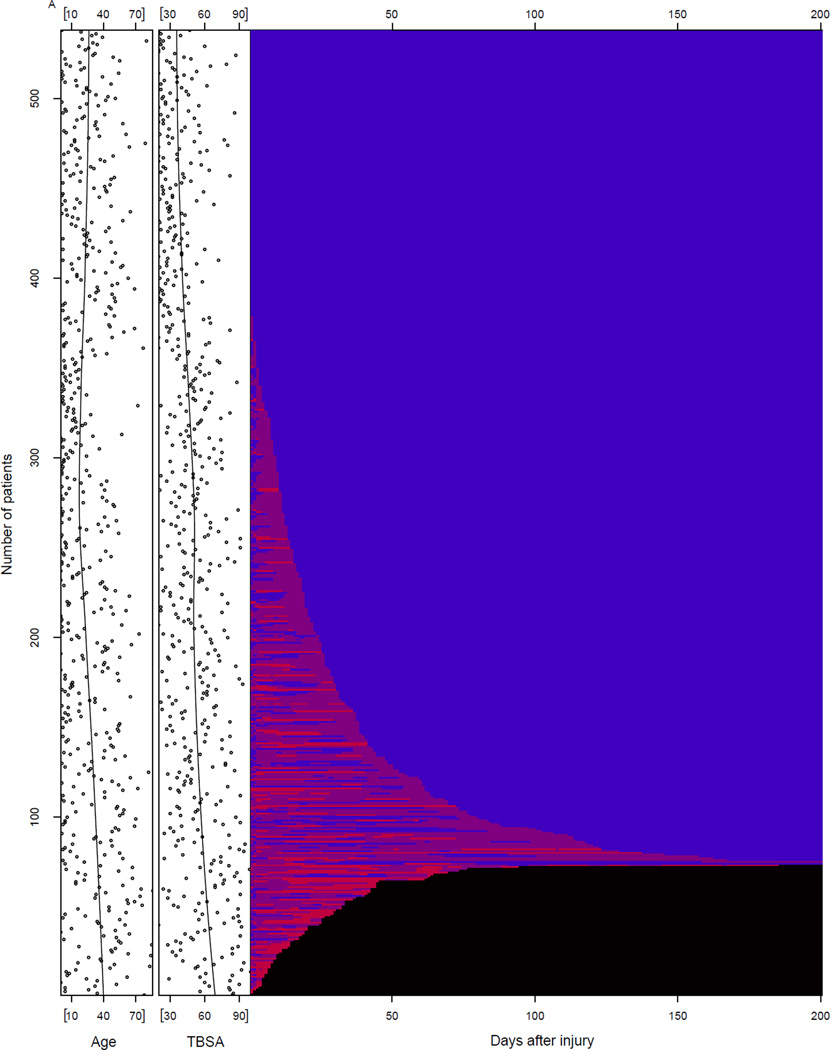
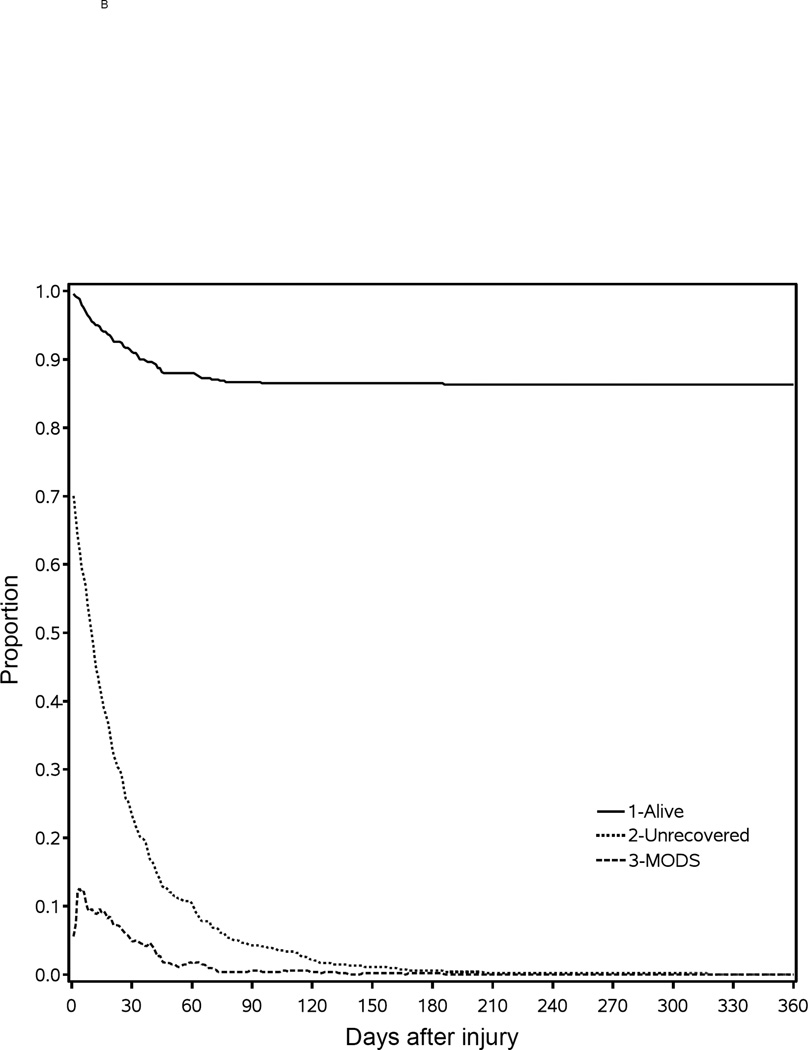
Results: Study patients were critically injured, as demonstrated by mean % total body surface area (TBSA) (41.2 ± 18.3 for adults and 57.8 ± 18.2 for children) and presence of inhalation injury in 38% of the adults and 54.8% of the children. Mortality in adults was 14.1% for those younger than 55 years and 38.5% for those aged 55 years and older. Mortality in patients younger than 17 years was 7.9%. Overall, the multiple organ failure rate was 27%. When controlling for age and % TBSA, presence of inhalation injury continues to be significant.
Conclusions: This study provides the current benchmark for major burn patients. Mortality rates, notwithstanding significant % TBSA and presence of inhalation injury, have significantly declined compared with previous benchmarks. Modern day surgical and medically intensive management has markedly improved to the point where we can expect patients younger than 55 years with severe burn injuries and inhalation injury to survive these devastating conditions.
Trial registration: ClinicalTrials.gov NCT00257244.
Conflict of interest statement
For all authors, none were declared.
Figures
Comment in
-
A multi-institutional benchmark of burn outcomes as a spur to further improvements in burn care.Ann Surg. 2014 May;259(5):842-3. doi: 10.1097/SLA.0000000000000664. Ann Surg. 2014. PMID: 24717373 No abstract available.
References
-
- National Hospital Ambulatory Medical Care Survey. [[cited July 24, 2013]];2010 Available from http://www.cdc.gov/nchs/ahcd/web_tables.htm#2010.
-
- Guidelines for the Operation of Burn Centers. American Burn Association. 2006 Available from http://www.ameriburn.org/verification_about.php.
-
- Finkelstein EA, Corso PS, Miller TR. Incidence and Economic Burden of Injuries in the United States. Oxford: Oxford University Press; 2006.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
