

Increased arterial stiffness in systemic lupus erythematosus (SLE) patients at low risk for cardiovascular disease: a cross-sectional controlled study
- PMID: 24722263
- PMCID: PMC3983200
- DOI: 10.1371/journal.pone.0094511
Increased arterial stiffness in systemic lupus erythematosus (SLE) patients at low risk for cardiovascular disease: a cross-sectional controlled study
Abstract
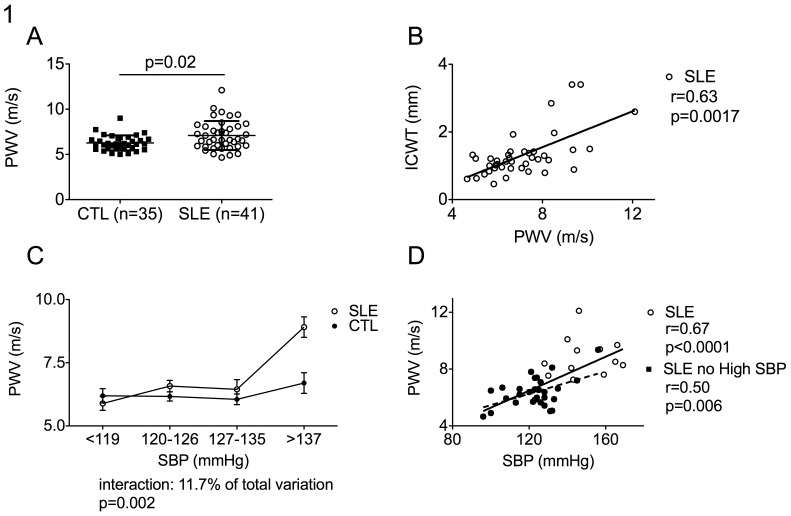
Cardiovascular disease (CVD) is a major cause of death in systemic lupus erythematosus (SLE) patients. Although the risk for cardiovascular events in patients with SLE is significant, the absolute number of events per year in any given cohort remains small. Thus, CVD risks stratification in patients with SLE focuses on surrogate markers for atherosclerosis at an early stage, such as reduced elasticity of arteries. Our study was designed to determine whether arterial stiffness is increased in SLE patients at low risk for CVD and analyze the role for traditional and non-traditional CVD risk factors on arterial stiffness in SLE. Carotid-femoral pulse wave velocity (PWV) was prospectively assessed as a measure of arterial stiffness in 41 SLE patients and 35 controls (CTL). Adjustment on age or Framingham score was performed using a logistic regression model. Factors associated with PWV were identified separately in SLE patients and in controls using Pearson's correlation coefficient for univariate analysis and multiple linear regression for multivariate analysis. SLE patients and controls displayed a low 10-year risk for CVD according to Framingham score (1.8±3.6% in SLE vs 1.6±2.8% in CTL, p = 0.46). Pulse wave velocity was, however, higher in SLE patients (7.1±1.6 m/s) as compared to controls (6.3±0.8 m/s; p = 0.01, after Framingham score adjustment) and correlated with internal carotid wall thickness (p = 0.0017). In multivariable analysis, only systolic blood pressure (p = 0.0005) and cumulative dose of glucocorticoids (p = 0.01) were associated with PWV in SLE patients. Interestingly, the link between systolic blood pressure (SBP) and arterial stiffness was also confirmed in SLE patients with normal systolic blood pressure. In conclusion, arterial stiffness is increased in SLE patients despite a low risk for CVD according to Framingham score and is associated with systolic blood pressure and glucocorticoid therapy.
Conflict of interest statement
Figures
References
-
- Esdaile JM, Abrahamowicz M, Grodzicky T, Li Y, Panaritis C, et al. (2001) Traditional Framingham risk factors fail to fully account for accelerated atherosclerosis in systemic lupus erythematosus. Arthritis and Rheumatism 44: 2331–2337. - PubMed
-
- Aranow C, Ginzler EM (2000) Epidemiology of cardiovascular disease in systemic lupus erythematosus. Lupus 9: 166–169. - PubMed
-
- Bjornadal L, Yin L, Granath F, Klareskog L, Ekbom A (2004) Cardiovascular disease a hazard despite improved prognosis in patients with systemic lupus erythematosus: results from a Swedish population based study 1964-95. The Journal of Rheumatology 31: 713–719. - PubMed
-
- Manzi S, Meilahn EN, Rairie JE, Conte CG, Medsger TA Jr, et al. (1997) Age-specific incidence rates of myocardial infarction and angina in women with systemic lupus erythematosus: comparison with the Framingham Study. American Journal of Epidemiology 145: 408–415. - PubMed
-
- Roman MJ, Shanker BA, Davis A, Lockshin MD, Sammaritano L, et al. (2003) Prevalence and correlates of accelerated atherosclerosis in systemic lupus erythematosus. The New England Journal of Medicine 349: 2399–2406. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
