

Critical findings: timing of notification in neuroradiology
- PMID: 24722306
- PMCID: PMC7964428
- DOI: 10.3174/ajnr.A3918
Critical findings: timing of notification in neuroradiology
Abstract
Background and purpose: Timely reporting of critical findings in radiology has been identified by The Joint Commission as one of the National Patient Safety Goals. Our aim was to determine the magnitude of delays between identifying a neuroradiologic critical finding and verbally notifying the caregiver in an effort to improve clinical outcomes.
Materials and methods: We surveyed the time of critical finding discovery, attempted notification, and direct communication between neuroradiologists and caregivers for weekday, evening, overnight, and weekend shifts during an 8-week period. The data were collected by trained observers and/or trainees and included 13 neuroradiology attendings plus fellows and residents. Critical findings were based on a previously approved 17-item list. Summary and comparative t test statistics were calculated, and sources of delays were identified.
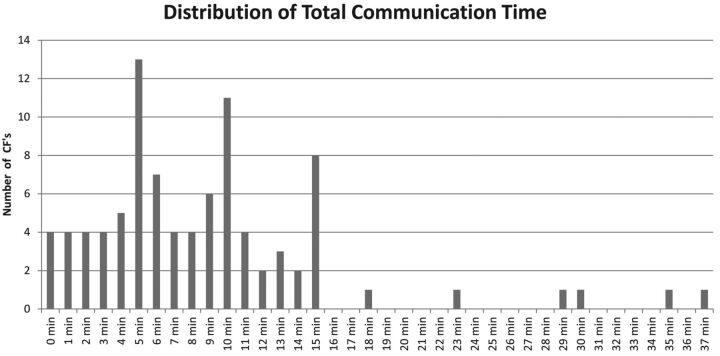
Results: Ninety-one critical findings were recorded. The mean time from study acquisition to critical finding discovery was 62.2 minutes, from critical finding discovery to call made 3.7 minutes, and from call made to direct communication, 5.2 minutes. The overall time from critical finding discovery to caregiver notification was within 10 minutes in 72.5% (66/91) and 15 minutes in 93.4% (85/91) of cases. There were no significant differences across shifts except for daytime versus overnight and weekend shifts, when means were 2.4, 5.6, and 8.7 minutes, respectively (P < .01). If >1 physician was called, the mean notification time increased from 3.5 to 10.1 minutes (P < .01). Sources of delays included inaccurate contact information, physician unavailability (shift change/office closed), patient transfer to a different service, or lack of responsiveness from caregivers.
Conclusions: Direct communication with the responsible referring physician occurred consistently within 10-15 minutes after observation of a critical finding. These delays are less than the average interval from study acquisition to critical finding discovery (mean, 62.2 minutes).
© 2014 by American Journal of Neuroradiology.
Figures
References
-
- The Joint Commission. National Patient Safety Goals. http://www.jointcommission.org/standards_information/npsgs.aspx. Accessed July 10, 2013
-
- American College of Radiology. ACR practice guidelines for communication of diagnostic imaging findings 2013. http://www.acr.org/∼/media/ACR/Documents/PGTS/guidelines/Comm_Diag_Imagi.... Accessed August 15, 2013
-
- Viertel VG, Trotter SA, Babiarz LS, et al. . Reporting of critical findings in neuroradiology. AJR Am J Roentgenol 2013;200:1132–37 - PubMed
-
- Trotter SA, Babiarz LS, Viertel VG, et al. . Determination and communication of critical findings in neuroradiology. J Am Coll Radiol 2013;10:45–50 - PubMed
-
- Anthony SG, Prevedello LM, Damiano MM, et al. . Impact of a 4-year quality improvement initiative to improve communication of critical imaging test results. Radiology 2011;259:802–07 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous