

A copeptin-based classification of the osmoregulatory defects in the syndrome of inappropriate antidiuresis
- PMID: 24722436
- PMCID: PMC4178436
- DOI: 10.1681/ASN.2013080895
A copeptin-based classification of the osmoregulatory defects in the syndrome of inappropriate antidiuresis
Abstract
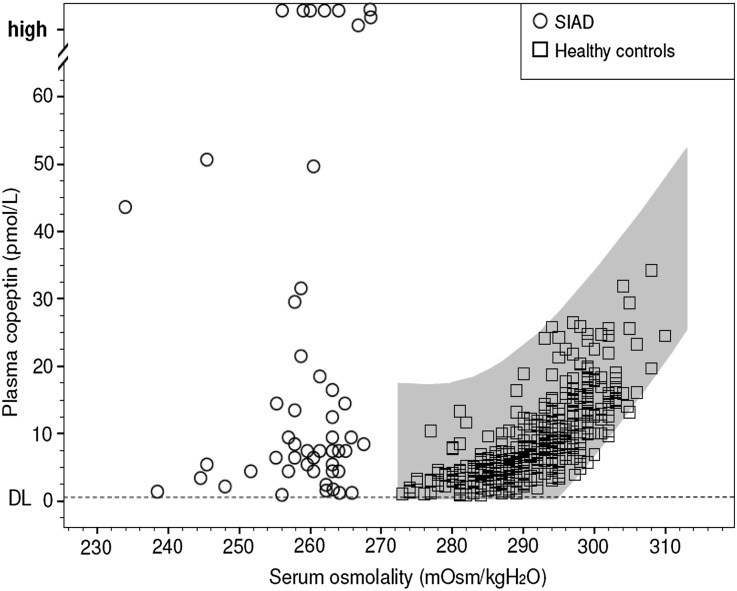
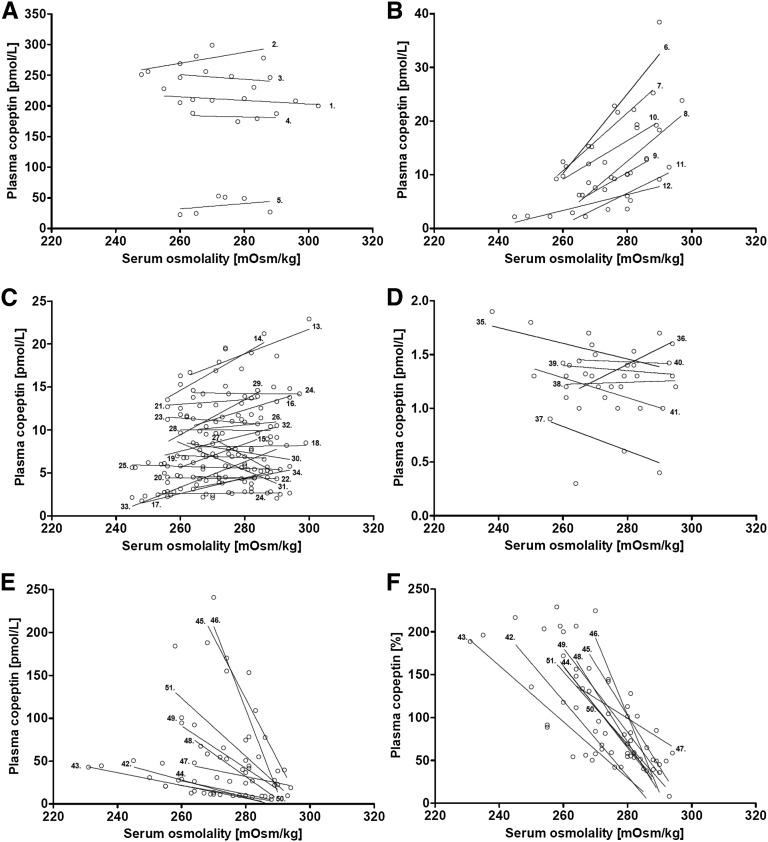
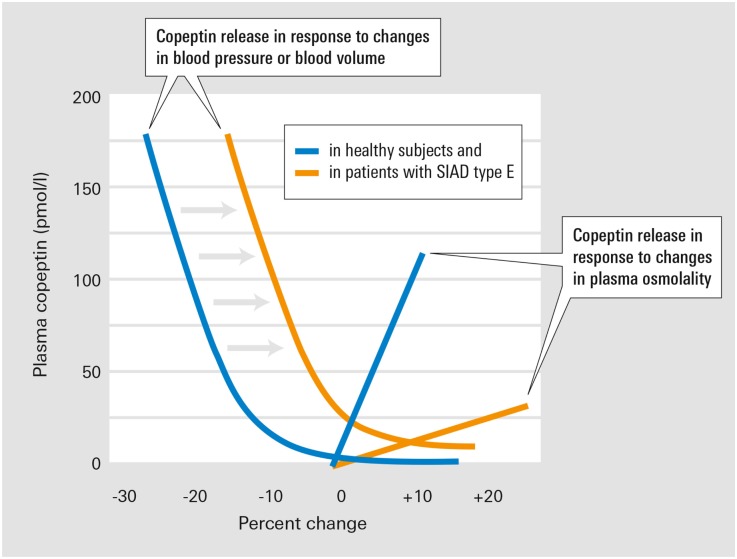
Hyponatremia, the most frequent electrolyte disorder, is caused predominantly by the syndrome of inappropriate antidiuresis (SIAD). A comprehensive characterization of SIAD subtypes, defined by type of osmotic dysregulation, is lacking, but may aid in predicting therapeutic success. Here, we analyzed serial measurements of serum osmolality and serum sodium, plasma arginine vasopressin (AVP), and plasma copeptin concentrations from 50 patients with hyponatremia who underwent hypertonic saline infusion. A close correlation between copeptin concentrations and serum osmolality existed in 68 healthy controls, with a mean osmotic threshold±SD of 282±4 mOsM/kg H2O. Furthermore, saline-induced changes in copeptin concentrations correlated with changes in AVP concentrations in controls and patients. With use of copeptin concentration as a surrogate measure of AVP concentration, patients with SIAD could be grouped according to osmoregulatory defect: Ten percent of patients had grossly elevated copeptin concentrations independent of serum osmolality (type A); 14% had copeptin concentrations that increased linearly with rising serum osmolality but had abnormally low osmotic thresholds (type B); 44% had normal copeptin concentrations independent of osmolality (type C), and 12% had suppressed copeptin concentrations independent of osmolality (type D). A novel SIAD subtype discovered in 20% of patients was characterized by a linear decrease in copeptin concentrations with increasing serum osmolality (type E or "barostat reset"). In conclusion, a partial or complete loss of AVP osmoregulation occurs in patients with SIAD. Although the mechanisms underlying osmoregulatory defects in individual patients are presumably diverse, we hypothesize that treatment responses and patient outcomes will vary according to SIAD subtype.
Copyright © 2014 by the American Society of Nephrology.
Figures
References
-
- Upadhyay A, Jaber BL, Madias NE: Incidence and prevalence of hyponatremia. Am J Med 119[Suppl 1]: S30–S35, 2006 - PubMed
-
- Klein L, O’Connor CM, Leimberger JD, Gattis-Stough W, Piña IL, Felker GM, Adams KF, Jr, Califf RM, Gheorghiade M, OPTIME-CHF Investigators : Lower serum sodium is associated with increased short-term mortality in hospitalized patients with worsening heart failure: results from the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME-CHF) study. Circulation 111: 2454–2460, 2005 - PubMed
-
- Schwartz WB, Bennett W, Curelop S, Bartter FC: A syndrome of renal sodium loss and hyponatremia probably resulting from inappropriate secretion of antidiuretic hormone. Am J Med 23: 529–542, 1957 - PubMed
-
- Zerbe R, Stropes L, Robertson G: Vasopressin function in the syndrome of inappropriate antidiuresis. Annu Rev Med 31: 315–327, 1980 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
