

Hepatic decompensation in antiretroviral-treated patients co-infected with HIV and hepatitis C virus compared with hepatitis C virus-monoinfected patients: a cohort study
- PMID: 24723077
- PMCID: PMC4254786
- DOI: 10.7326/M13-1829
Hepatic decompensation in antiretroviral-treated patients co-infected with HIV and hepatitis C virus compared with hepatitis C virus-monoinfected patients: a cohort study
Abstract
Background: The incidence and determinants of hepatic decompensation have been incompletely examined among patients co-infected with HIV and hepatitis C virus (HCV) in the antiretroviral therapy (ART) era, and few studies have compared outcome rates with those of patients with chronic HCV alone.
Objective: To compare the incidence of hepatic decompensation between antiretroviral-treated patients co-infected with HIV and HCV and HCV-monoinfected patients and to evaluate factors associated with decompensation among co-infected patients receiving ART.
Design: Retrospective cohort study.
Setting: Veterans Health Administration.
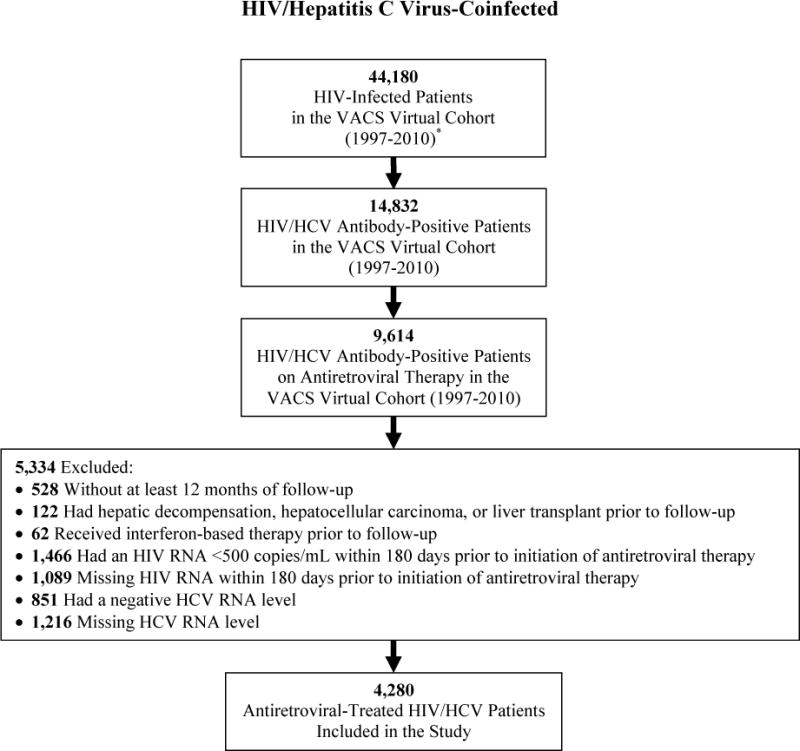
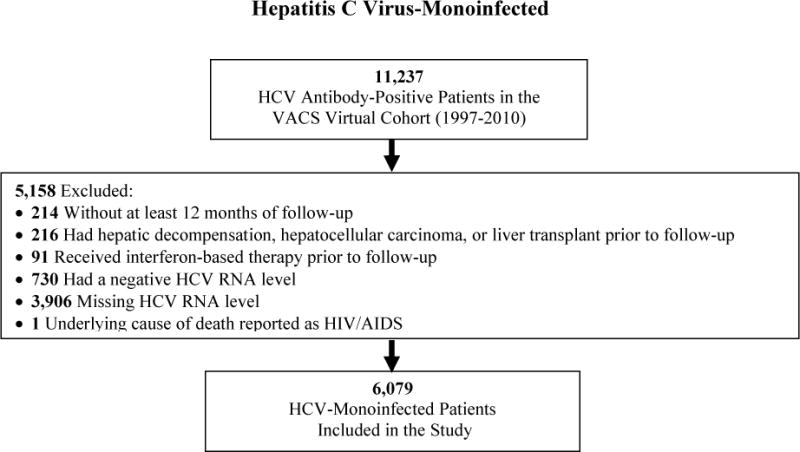
Patients: 4280 co-infected patients who initiated ART and 6079 HCV-monoinfected patients receiving care between 1997 and 2010. All patients had detectable HCV RNA and were HCV treatment-naive.
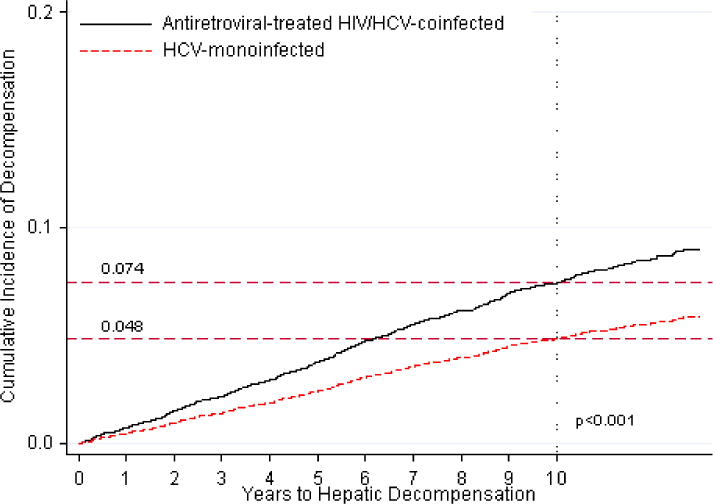
Measurements: Incident hepatic decompensation, determined by diagnoses of ascites, spontaneous bacterial peritonitis, or esophageal variceal hemorrhage.
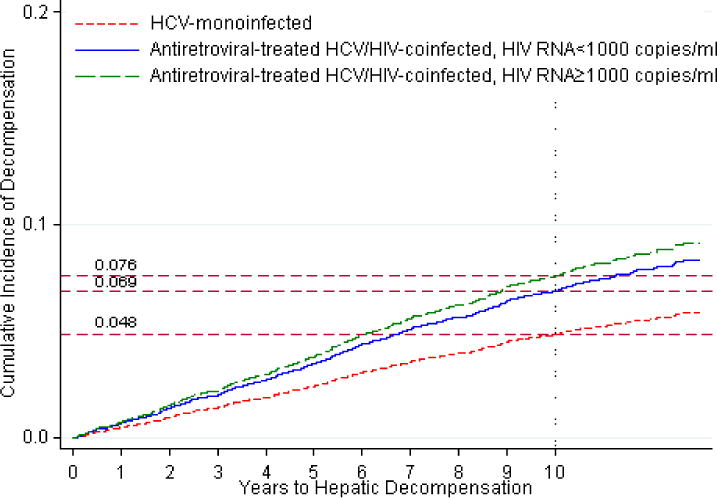
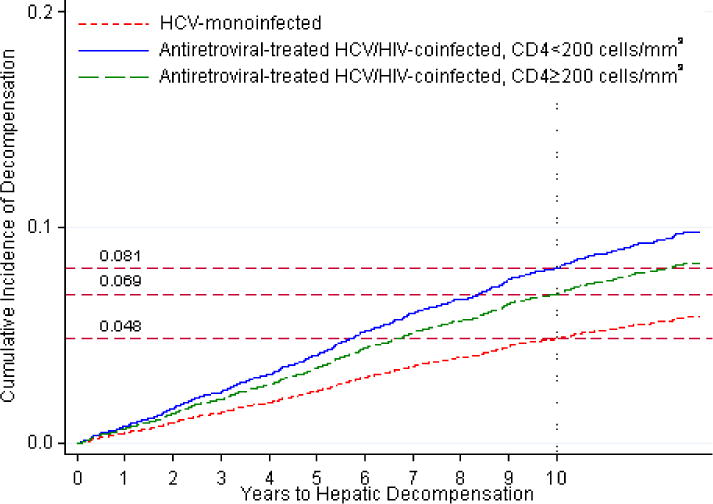
Results: The incidence of hepatic decompensation was greater among co-infected than monoinfected patients (7.4% vs. 4.8% at 10 years; P < 0.001). Compared with HCV-monoinfected patients, co-infected patients had a higher rate of hepatic decompensation (hazard ratio [HR] accounting for competing risks, 1.56 [95% CI, 1.31 to 1.86]). Co-infected patients who maintained HIV RNA levels less than 1000 copies/mL still had higher rates of decompensation than HCV-monoinfected patients (HR, 1.44 [CI, 1.05 to 1.99]). Baseline advanced hepatic fibrosis (FIB-4 score >3.25) (HR, 5.45 [CI, 3.79 to 7.84]), baseline hemoglobin level less than 100 g/L (HR, 2.24 [CI, 1.20 to 4.20]), diabetes mellitus (HR, 1.88 [CI, 1.38 to 2.56]), and nonblack race (HR, 2.12 [CI, 1.65 to 2.72]) were each associated with higher rates of decompensation among co-infected patients.
Limitation: Observational study of predominantly male patients.
Conclusion: Despite receiving ART, patients co-infected with HIV and HCV had higher rates of hepatic decompensation than HCV-monoinfected patients. Rates of decompensation were higher for co-infected patients with advanced liver fibrosis, severe anemia, diabetes, and nonblack race.
Primary funding source: National Institutes of Health.
Conflict of interest statement
Figures
References
-
- Sherman KE, Rouster SD, Chung RT, Rajicic N. Hepatitis C virus prevalence among patients infected with human immunodeficiency virus: a cross-sectional analysis of the US adult AIDS Clinical Trials Group. Clin Infect Dis. 2002;34(6):831–7. - PubMed
-
- Frederick T, Burian P, Terrault N, Cohen M, Augenbraun M, Young M, et al. Factors associated with prevalent hepatitis C infection among HIV-infected women with no reported history of injection drug use: the Women’s Interagency HIV Study (WIHS) AIDS Patient Care STDS. 2009;23(11):915–23. - PMC - PubMed
-
- Raymond HF, Hughes A, O’Keefe K, Stall RD, McFarland W. Hepatitis C prevalence among HIV-positive MSM in San Francisco: 2004 and 2008. Sex Transm Dis. 2011;38(3):219–20. - PubMed
-
- Benhamou Y, Bochet M, Di Martino V, Charlotte F, Azria F, Coutellier A, et al. Liver fibrosis progression in human immunodeficiency virus and hepatitis C virus coinfected patients. The Multivirc Group. Hepatology. 1999;30(4):1054–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical