

Hospital costs of total hip arthroplasty for developmental dysplasia of the hip
- PMID: 24723141
- PMCID: PMC4048391
- DOI: 10.1007/s11999-014-3587-9
Hospital costs of total hip arthroplasty for developmental dysplasia of the hip
Abstract
Background: Developmental dysplasia of the hip (DDH) is a leading cause of total hip arthroplasty (THA) in younger patients. It is unknown how the hospital costs of THA in patients with DDH compare with patients with degenerative arthritis.
Questions/purposes: We undertook this study to determine (1) the hospital cost and length of stay associated with primary THA in patients with dysplasia compared with nondysplastic control subjects; (2) the hospital cost and length of stay of THA in severely dysplastic hips compared with mildly dysplastic hips; and (3) perioperative complications in patients with DDH compared with patients without dysplasia.
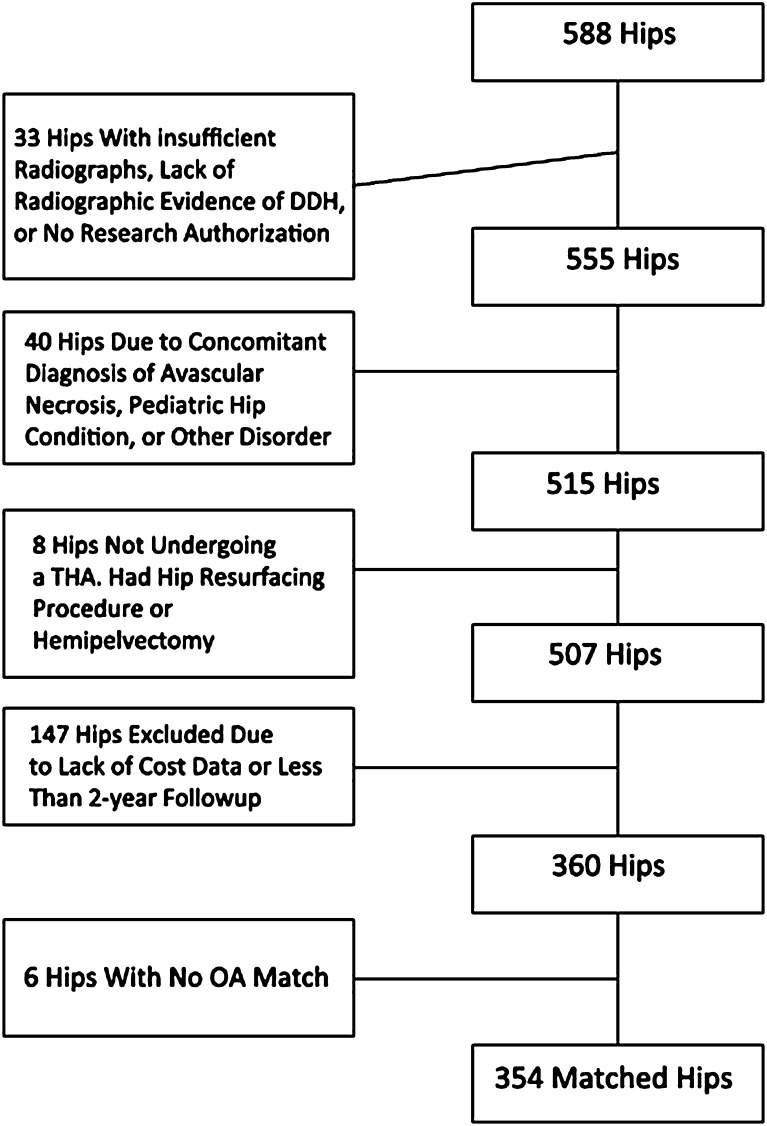
Methods: This matched-cohort study included 354 patients undergoing primary THA for DDH and 1029 age-, sex-, and calendar year-matched patients undergoing THA for primary osteoarthritis between 2000 and 2008. DDH severity was measured by the Crowe classification. An institutional database was used to calculate the cost of care. Using line item details (date, type, frequency, and billed charge) for every procedure or service billed at our institution for each patient, bottom-up microcosting valuation techniques were used to generate standardized inflation-adjusted estimates of the cost of each service or procedure in constant dollars. Generalized linear random effects models were used to compare length of stay and costs during hospitalization and the 90-day period after surgery. Query of a longitudinal institutional database was used to identify documented complications.
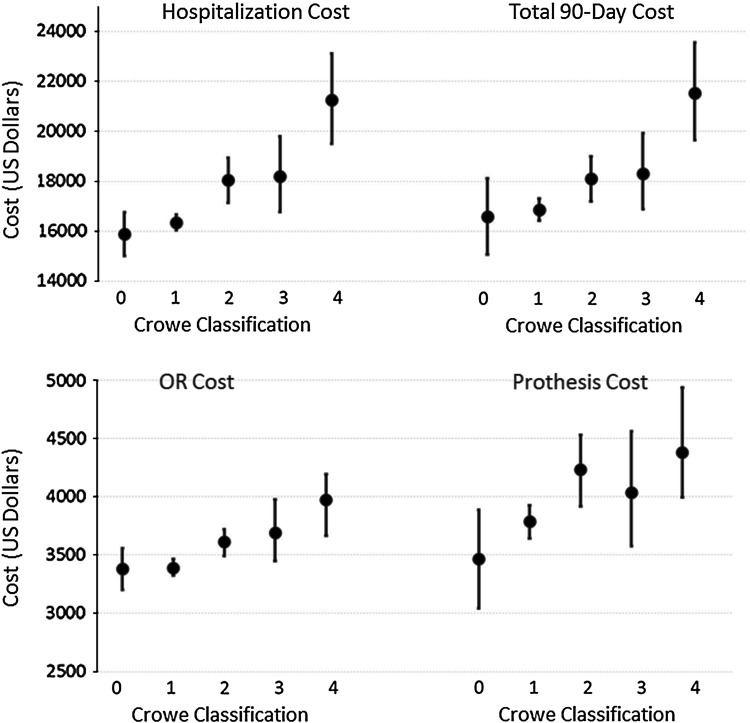
Results: Patients with DDH undergoing primary THA incurred higher hospital costs than patients with primary osteoarthritis (USD 16,949 versus USD 16,485, p = 0.012). Operating room costs (USD 3471 versus USD 3417, p = 0.0085) and implant costs (USD 3896 versus USD 3493, p < 0.001) were higher in the DDH group compared with the osteoarthritis group. Length of stay was not different between the two groups (4 versus 4 days, p = 0.46). Crowe 4 hips had higher hospital costs than Crowe 1 hips (USD 21,246 versus USD 16,345, p < 0.001) with an associated longer length of stay (5 days versus 4 days, p = 0.0011) and higher implant costs (USD 4380 versus USD 3788, p = 0.0012). There was no detectible difference in 90-day complications in the case group compared with patients undergoing THA for osteoarthritis.
Conclusions: Hospital cost of primary THA is approximately USD 450 higher in patients with DDH compared with osteoarthritis. Increased severity of dysplasia (Crowe classification) was associated with higher costs.
Level of evidence: Level IV, economic and decision analyses. See Guidelines for Authors for a complete description of levels of evidence.
Figures

References
-
- Crowe JF, Mani VJ, Ranawat CS. Total hip replacement in congenital dislocation and dysplasia of the hip. J Bone Joint Surg Am. 1979;61:15–23. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
