

Clarithromycin overcomes resistance to lenalidomide and dexamethasone in multiple myeloma
- PMID: 24723438
- PMCID: PMC4390045
- DOI: 10.1002/ajh.23733
Clarithromycin overcomes resistance to lenalidomide and dexamethasone in multiple myeloma
Abstract
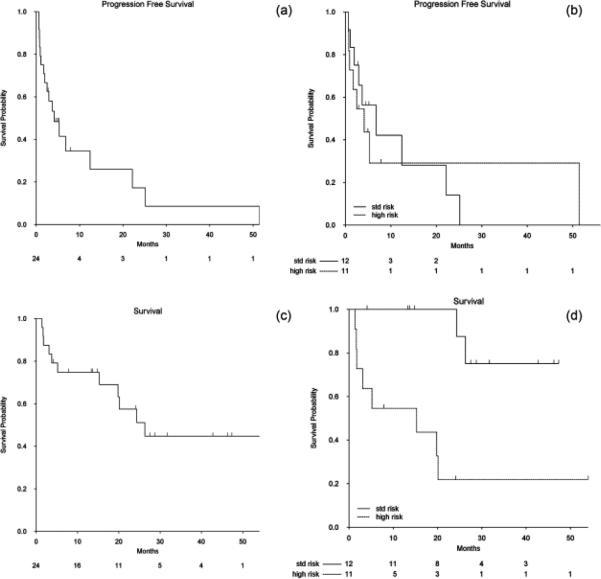
The combination of clarithromycin, lenalidomide and dexamethasone (BiRd) has led to highly durable responses in newly diagnosed myeloma. However, the ability of clarithromycin to overcome resistance to lenalidomide and dexamethasone (Rd) is not known. To study this, we performed a retrospective analysis of 24 patients with myeloma for which clarithromycin was added to Rd at the time of progression on Rd. The median number of prior therapies was 3 (range 1-8). The best response was complete response (CR) in one (4.2%), very good partial response (VGPR) in one (4.2%) and partial response in eight (33.3%) patients. Ten patients, 41.7% (95% CI: 22.1, 63.4), achieved ≥PR. The median time to response was 4.4 months (range 1-13.6 months) and the median duration of response was 6.9 months (range 3-52.2 months). The clinical benefit rate (CR + VGPR + PR + MR) was 45.8% (95% CI 25.6, 67.2). The median progression-free survival was 4 months. Median overall survival was 25 months with a median follow-up of 27.5 months. The regimen was well tolerated and only 2 patients needed a clarithromycin dose reduction. Addition of clarithromycin to Rd can overcome resistance to Rd in a subset of patients and lead to durable clinical responses.
© 2014 Wiley Periodicals, Inc.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Palumbo A, Anderson K. Multiple myeloma. N Engl J Med. 2011;364:1046–1060. - PubMed
-
- Brenner H, Gondos A, Pulte D. Recent major improvement in long-term survival of younger patients with multiple myeloma. Blood. 2008;111:2521–2526. - PubMed
-
- Coleman M, Leonard J, Lyons L, Pekle K, Nahum K, Pearse R, Niesvizky R, Michaeli J. BLT-D (clarithromycin [Biaxin], low-dose thalidomide, and dexamethasone) for the treatment of myeloma and Waldenstrom’s macroglobulinemia. Leuk Lymphoma. 2002;43:1777–1782. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous