

Incidence and relative survival of anaplastic astrocytomas
- PMID: 24723565
- PMCID: PMC4165416
- DOI: 10.1093/neuonc/nou053
Incidence and relative survival of anaplastic astrocytomas
Abstract
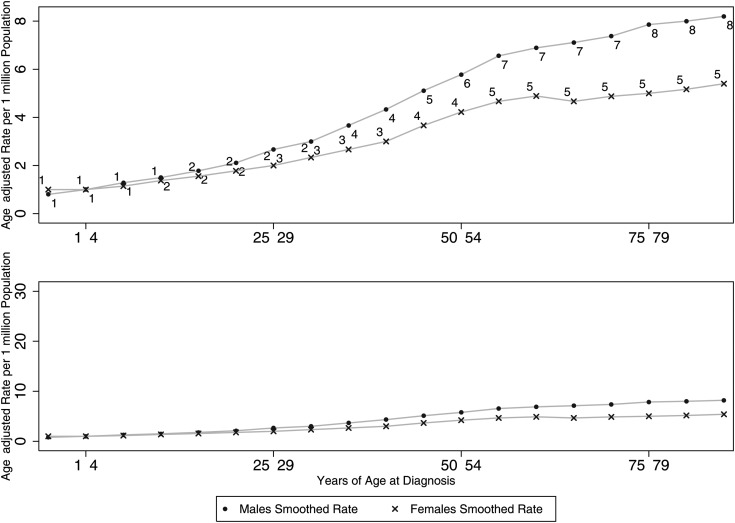
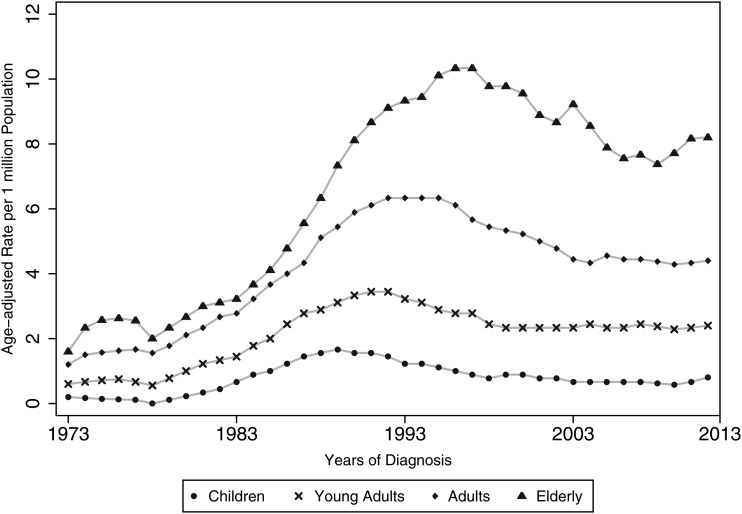
Background: The purpose of this study was to investigate the relationship between age and the incidence and relative survival of anaplastic astrocytoma (AA).
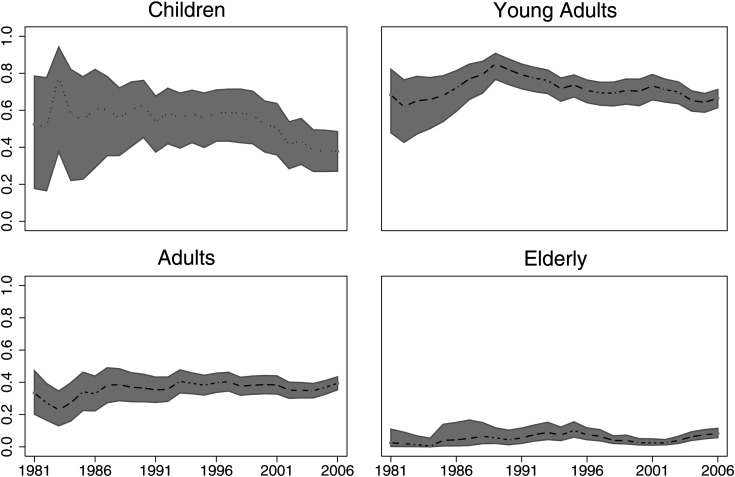
Methods: Data from the Surveillance, Epidemiology and End Results database were used to identify 3202 patients with AA. These data were analyzed to assess incidence rates, relative survival, and the standardized mortality ratio across age groups. Time trends were modeled using delayed-entry modeling.
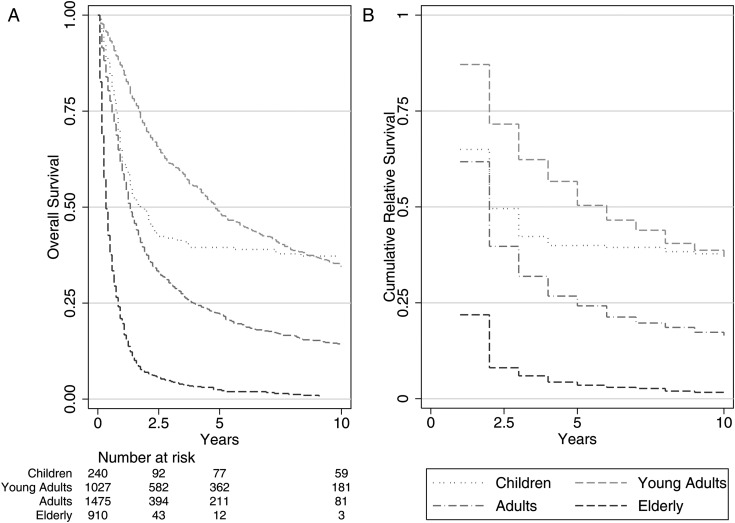
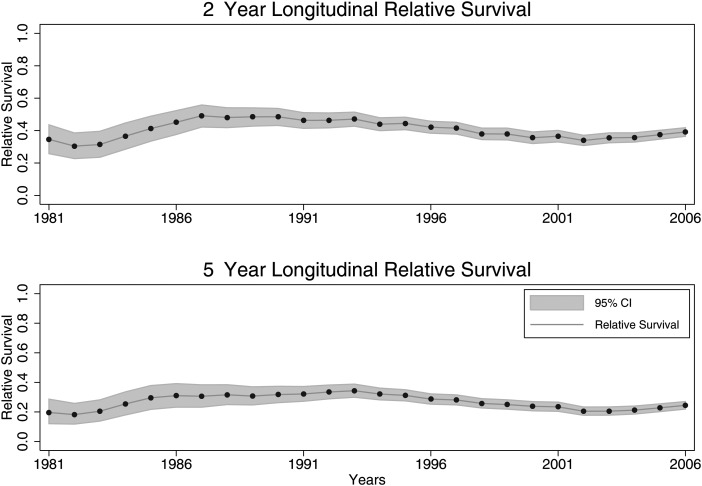
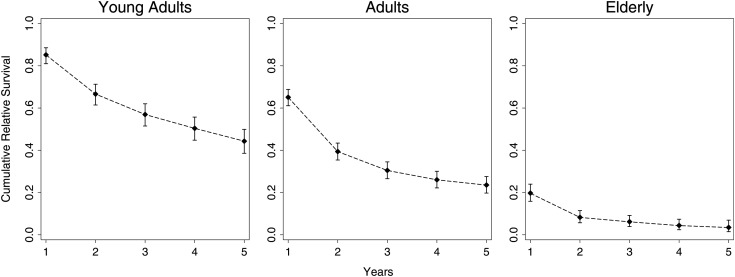
Results: The overall incidence of AA was an age-adjusted rate of 3.5 per million person/years. The overall age-standardized 5- and 10-year relative survival rates of populations with AA were 23.6% and 15.1%, respectively. The overall standardized mortality ratio for the entire cohort was 46 (95% confidence interval: 45, 48).
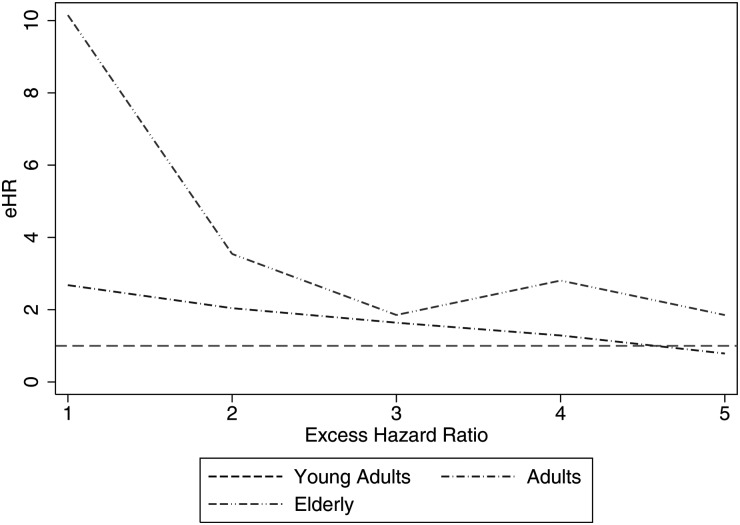
Conclusions: Patients with a diagnosis of AA are 46 times more likely to die than persons matched for age/sex/year of the general population. The effect of age on survival is present for only the first 2 years postdiagnosis. Measuring the effect of age on survival for populations with an AA is not amenable to using models with proportional hazards as an assumption because of the presence of a reverse fork-type interaction.
Keywords: anaplastic astrocytoma; brain tumor; nonproportional hazards; relative survival; standardized mortality ratio.
© The Author(s) 2014. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Australian Institute of Health and Welfare. Cancer Survival and Prevalence in Australia: Period Estimates From 1982 to 2010. Canberra: AIHW; 2012. - PubMed
-
- Horner MJRL, Krapcho M, Neyman N, et al. SEER Cancer Statistics Review 1975–2006. http://seer.cancer.gov/csr/1975_2006/ based on November 2008 SEER data submission, posted to the SEER web site, 2009.
-
- Radhakrishnan K, Mokri B, Parisi JE, et al. The trends in incidence of primary brain tumors in the population of Rochester, Minnesota. Ann Neurol. 1995;37(1):67–73. - PubMed
-
- Smoll NR, Drummond KJ. The incidence of medulloblastomas and primitive neurectodermal tumours in adults and children. J Clin Neurosci. 2012;19(11):1541–1544. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
