

Induced pluripotent stem cells for post-myocardial infarction repair: remarkable opportunities and challenges
- PMID: 24723658
- PMCID: PMC4016859
- DOI: 10.1161/CIRCRESAHA.114.300556
Induced pluripotent stem cells for post-myocardial infarction repair: remarkable opportunities and challenges
Abstract
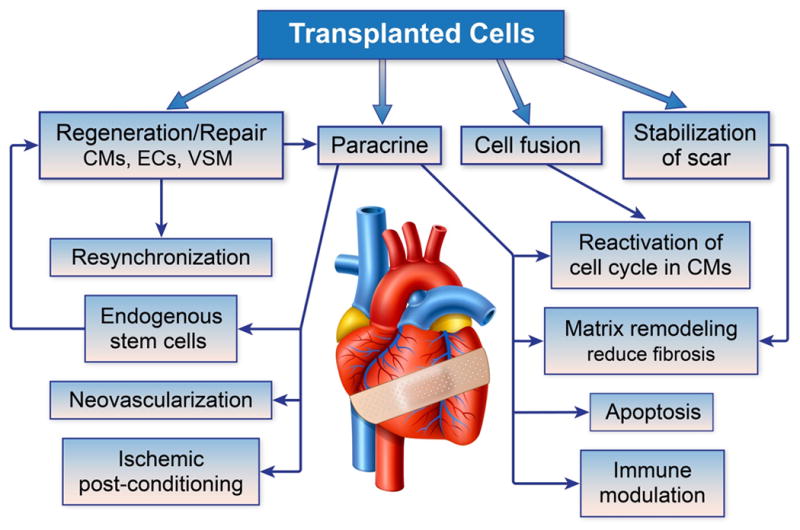
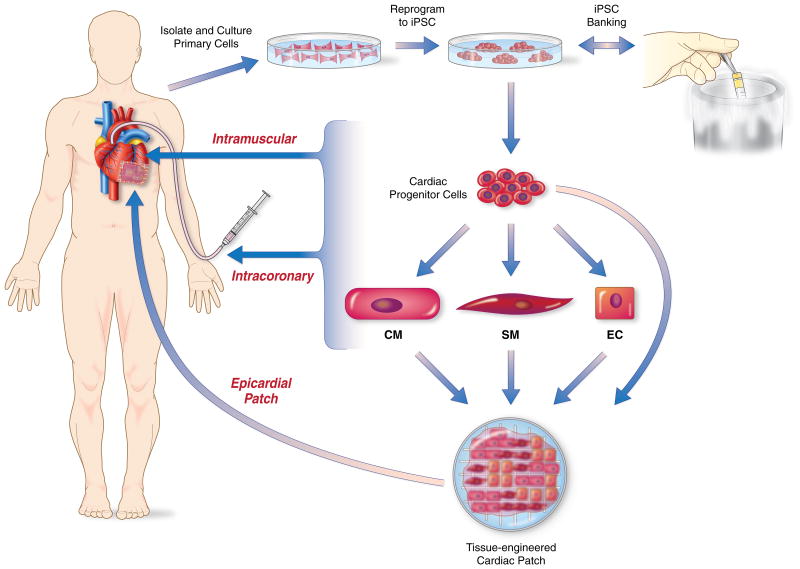
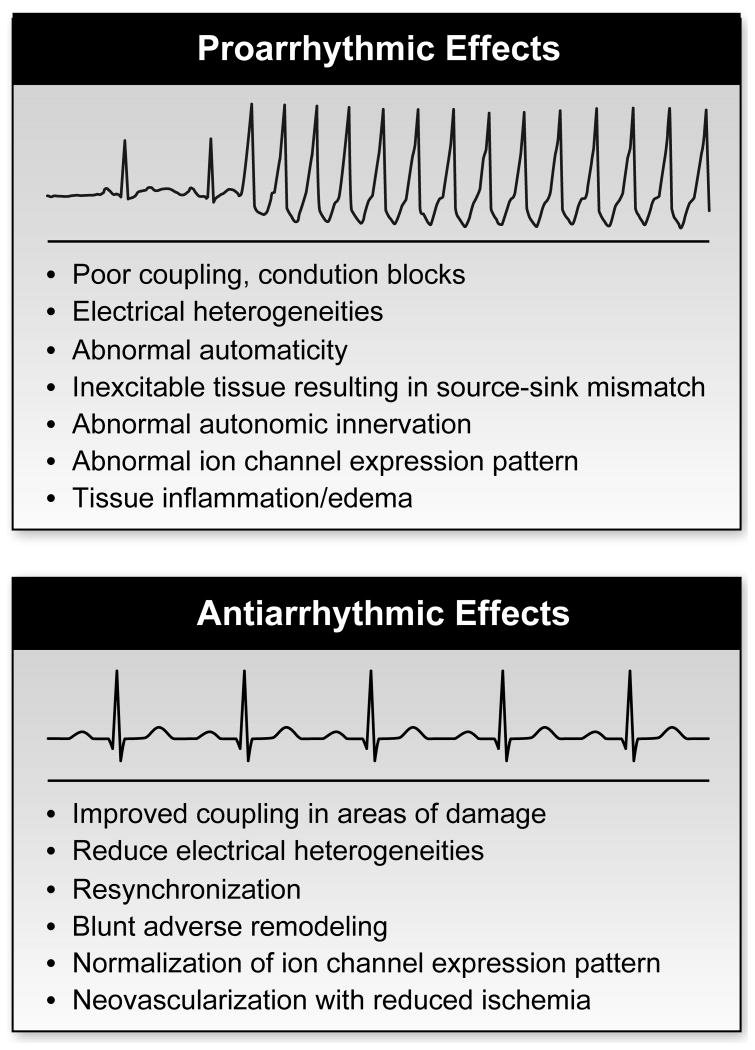
Coronary artery disease with associated myocardial infarction continues to be a major cause of death and morbidity around the world, despite significant advances in therapy. Patients who have large myocardial infarctions are at highest risk for progressive heart failure and death, and cell-based therapies offer new hope for these patients. A recently discovered cell source for cardiac repair has emerged as a result of a breakthrough reprogramming somatic cells to induced pluripotent stem cells (iPSCs). The iPSCs can proliferate indefinitely in culture and can differentiate into cardiac lineages, including cardiomyocytes, smooth muscle cells, endothelial cells, and cardiac progenitors. Thus, large quantities of desired cell products can be generated without being limited by cellular senescence. The iPSCs can be obtained from patients to allow autologous therapy or, alternatively, banks of human leukocyte antigen diverse iPSCs are possible for allogeneic therapy. Preclinical animal studies using a variety of cell preparations generated from iPSCs have shown evidence of cardiac repair. Methodology for the production of clinical grade products from human iPSCs is in place. Ongoing studies for the safety of various iPSC preparations with regard to the risk of tumor formation, immune rejection, induction of arrhythmias, and formation of stable cardiac grafts are needed as the field advances toward the first-in-man trials of iPSCs after myocardial infarction.
Keywords: cell- and tissue-based therapy; induced pluripotent stem cell; myocardial infarction; regenerative medicine; tissue engineering.
Figures
References
-
- Orlic D, Kajstura J, Chimenti S, Jakoniuk I, Anderson SM, Li B, Pickel J, McKay R, Nadal-Ginard B, Bodine DM, Leri A, Anversa P. Bone marrow cells regenerate infarcted myocardium. Nature. 2001;410:701–705. - PubMed
-
- Murry CE, Soonpaa MH, Reinecke H, Nakajima H, Nakajima HO, Rubart M, Pasumarthi KB, Virag JI, Bartelmez SH, Poppa V, Bradford G, Dowell JD, Williams DA, Field LJ. Haematopoietic stem cells do not transdifferentiate into cardiac myocytes in myocardial infarcts. Nature. 2004;428:664–668. - PubMed
-
- Balsam LB, Wagers AJ, Christensen JL, Kofidis T, Weissman IL, Robbins RC. Haematopoietic stem cells adopt mature haematopoietic fates in ischaemic myocardium. Nature. 2004;428:668–673. - PubMed
-
- Lunde K, Solheim S, Aakhus S, Arnesen H, Abdelnoor M, Egeland T, Endresen K, Ilebekk A, Mangschau A, Fjeld JG, Smith HJ, Taraldsrud E, Grogaard HK, Bjornerheim R, Brekke M, Muller C, Hopp E, Ragnarsson A, Brinchmann JE, Forfang K. Intracoronary injection of mononuclear bone marrow cells in acute myocardial infarction. N Engl J Med. 2006;355:1199–1209. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
