

Evaluation of Pharyngeal Function between No Bolus and Bolus Propofol Induced Sedation for Advanced Upper Endoscopy
- PMID: 24723747
- PMCID: PMC3958785
- DOI: 10.1155/2014/248097
Evaluation of Pharyngeal Function between No Bolus and Bolus Propofol Induced Sedation for Advanced Upper Endoscopy
Abstract
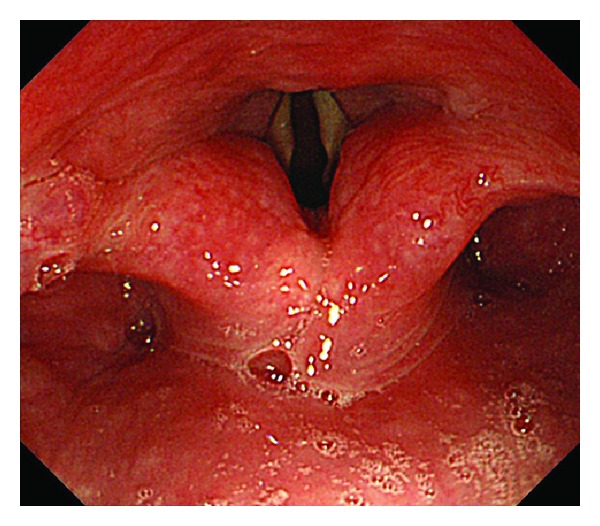
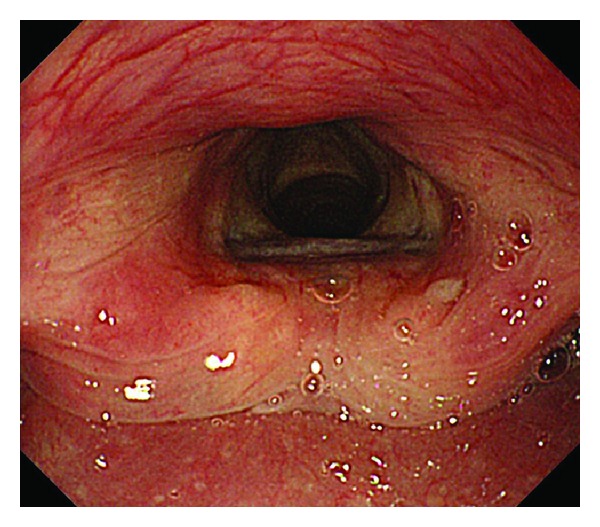
This study aimed to assess pharyngeal function between no bolus and bolus propofol induced sedation during gastric endoscopic submucosal dissection. A retrospective study was conducted involving consecutive gastric cancer patients. Patients in the no bolus group received a 3 mg/kg/h maintenance dose of propofol after the initiation of sedation without bolus injection. All patients in the bolus group received the same maintenance dose of propofol with bolus 0.5 mg/kg propofol injection. Pharyngeal functions were evaluated endoscopically for the first 5 min following the initial administration of propofol. Fourteen patients received no bolus propofol induction and 13 received bolus propofol induction. Motionless vocal cords were observed in 2 patients (14%) in the no bolus group and 3 (23%) in the bolus group. Trachea cartilage was not observed in the no bolus group but was apparent in 6 patients (46%) in the bolus group (P < 0.01). Scope stimulated pharyngeal reflex was observed in 11 patients (79%) in the no bolus group and in 3 (23%) in the bolus group (P < 0.01). Propofol induced sedation without bolus administration preserves pharyngeal function and may constitute a safer sedation method than with bolus.
Figures
Similar articles
-
Continuous infusion versus intermittent bolus injection of propofol during endoscopic retrograde cholangiopancreatography.Korean J Intern Med. 2020 Nov;35(6):1338-1345. doi: 10.3904/kjim.2018.233. Epub 2020 Mar 5. Korean J Intern Med. 2020. PMID: 32126750 Free PMC article.
-
Safe and effective sedation in endoscopic submucosal dissection for early gastric cancer: a randomized comparison between propofol continuous infusion and intermittent midazolam injection.J Gastroenterol. 2010 Aug;45(8):831-7. doi: 10.1007/s00535-010-0222-8. Epub 2010 Mar 13. J Gastroenterol. 2010. PMID: 20228999 Clinical Trial.
-
Intermittent manually controlled versus continuous infusion of propofol for deep sedation during interventional endoscopy: a prospective randomized trial.Scand J Gastroenterol. 2012 Sep;47(8-9):1078-85. doi: 10.3109/00365521.2012.685758. Epub 2012 May 28. Scand J Gastroenterol. 2012. PMID: 22631051 Clinical Trial.
-
Bispectral index as a guide for titration of propofol during procedural sedation among children.Pediatrics. 2005 Jun;115(6):1666-74. doi: 10.1542/peds.2004-1979. Pediatrics. 2005. PMID: 15930231 Review.
-
Comparison of bolus versus continuous infusion of propofol for procedural sedation: a meta-analysis.Curr Med Res Opin. 2017 Nov;33(11):1935-1943. doi: 10.1080/03007995.2017.1370419. Epub 2017 Sep 1. Curr Med Res Opin. 2017. PMID: 28859533 Review.
Cited by
-
Propofol sedation during endoscopic treatment for early gastric cancer compared to midazolam.World J Gastroenterol. 2014 Sep 14;20(34):11985-90. doi: 10.3748/wjg.v20.i34.11985. World J Gastroenterol. 2014. PMID: 25232235 Free PMC article. Review.
-
Anesthetic effect of different doses of butorphanol in patients undergoing gastroscopy and colonoscopy.BMC Surg. 2021 May 27;21(1):266. doi: 10.1186/s12893-021-01262-8. BMC Surg. 2021. PMID: 34044830 Free PMC article. Clinical Trial.
-
Comparison of the efficacy and safety of sedation between dexmedetomidine-remifentanil and propofol-remifentanil during endoscopic submucosal dissection.World J Gastroenterol. 2015 Mar 28;21(12):3671-8. doi: 10.3748/wjg.v21.i12.3671. World J Gastroenterol. 2015. PMID: 25834336 Free PMC article. Clinical Trial.
-
Continuous infusion versus intermittent bolus injection of propofol during endoscopic retrograde cholangiopancreatography.Korean J Intern Med. 2020 Nov;35(6):1338-1345. doi: 10.3904/kjim.2018.233. Epub 2020 Mar 5. Korean J Intern Med. 2020. PMID: 32126750 Free PMC article.
References
-
- Gotoda T, Yamamoto H, Soetikno RM. Endoscopic submucosal dissection of early gastric cancer. Journal of Gastroenterology. 2006;41(10):929–942. - PubMed
-
- Oda I, Gotoda T, Hamanaka H, et al. Endoscopic submucosal dissection for early gastric cancer: technical feasibility, operation time and complications from a large consecutive series. Digestive Endoscopy. 2005;17(1):54–58.
-
- Kiriyama S, Gotoda T, Sano H, et al. Safe and effective sedation in endoscopic submucosal dissection for early gastric cancer: a randomized comparison between propofol continuous infusion and intermittent midazolam injection. Journal of Gastroenterology. 2010;45:831–837. - PubMed
-
- Vargo JJ, Zuccaro G, Jr., Dumot JA, et al. Gastroenterologist-administered propofol versus meperidine and midazolam for advanced upper endoscopy: a prospective, randomized trial. Gastroenterology. 2002;123(1):8–16. - PubMed
-
- Dewitt J, McGreevy K, Sherman S, Imperiale TF. Nurse-administered propofol sedation compared with midazolam and meperidine for EUS: a prospective, randomized trial. Gastrointestinal Endoscopy. 2008;68(3):499–509. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources