

Immune cell infiltration patterns and survival in head and neck squamous cell carcinoma
- PMID: 24723971
- PMCID: PMC3979926
Immune cell infiltration patterns and survival in head and neck squamous cell carcinoma
Abstract
Purpose: This study examines the tumour-host immune interactions in head and neck squamous cell carcinoma (HNSCC) and their relationship to human papillomavirus (HPV) infectivity and patient survival.
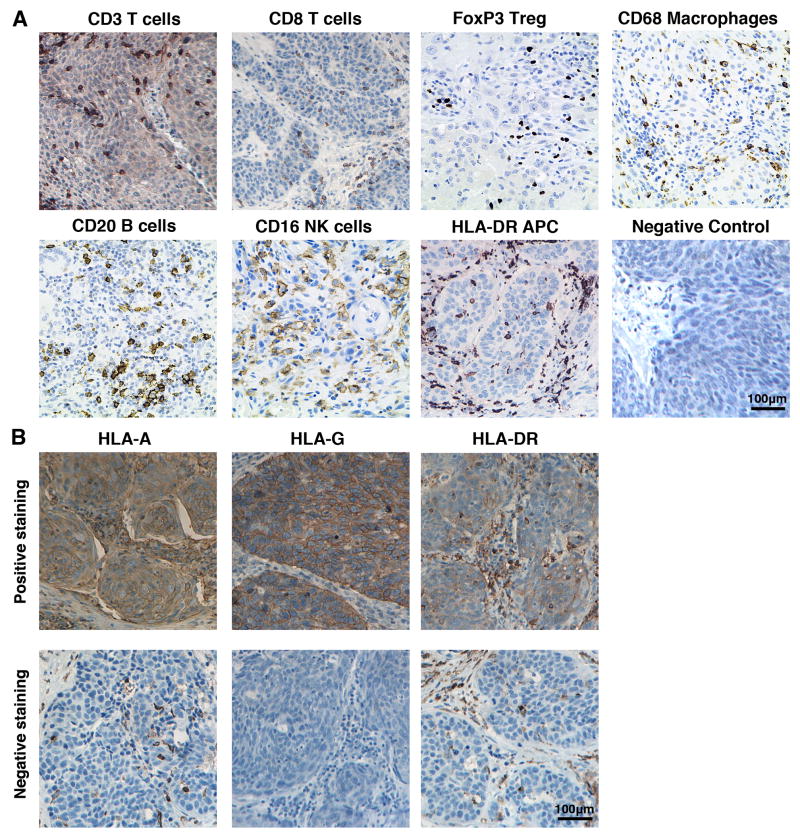
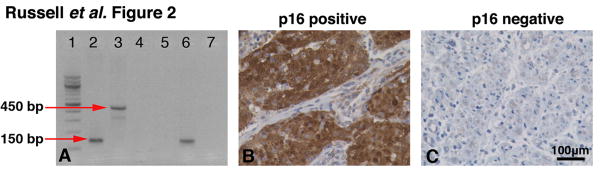
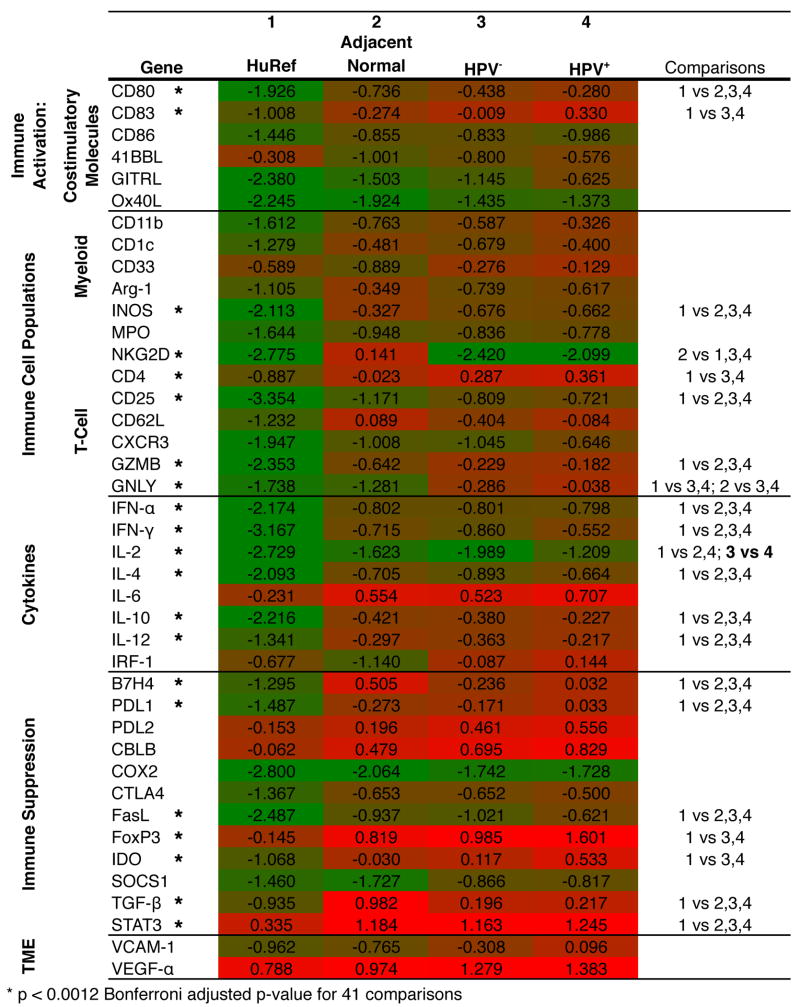
Methods: The adaptive and innate immune profile of surgical tumour specimens obtained from HNSCC patients was determined using qRT-PCR and immunohistochemistry. Intratumoural and invading margin leukocyte populations (CD3, CD8, CD16, CD20, CD68, FoxP3 and HLA-DR) were quantified and compared with patient disease-specific survival. Additionally, the expression of 41 immune activation- and suppression-related genes was evaluated in the tumour microenvironment. Tumour cells were also assessed for expression of HLA-A, HLA-G and HLA-DR. HPV infectivity of tumour biopsies was determined using HPV consensus primers (MY09/MY11 and GP5+/GP6+) and confirmed with p16 immunohistochemistry.
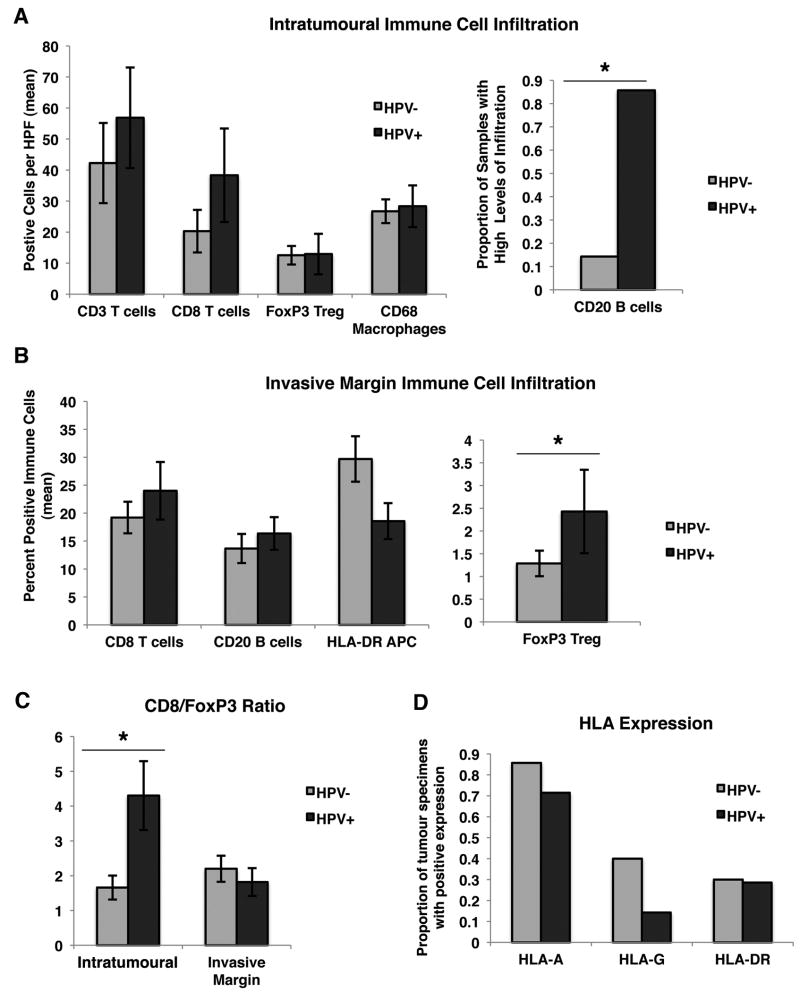
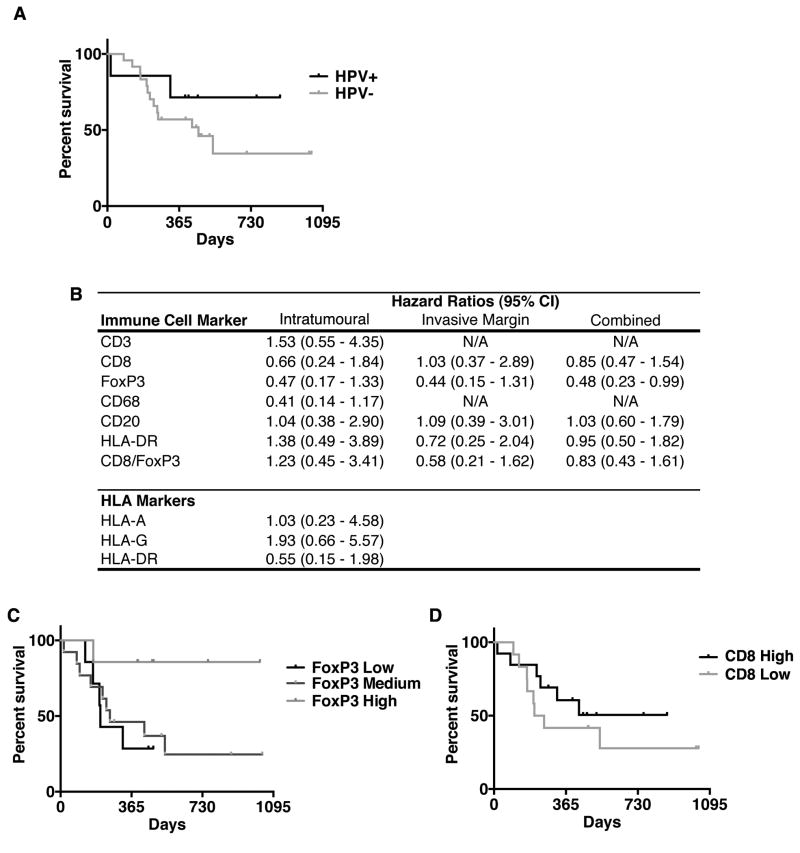
Results: HPV+ patient samples showed a significantly increased infiltration by intratumoural CD20+ B cells, as well as by invasive margin FoxP3+Treg, compared with HPV- patient samples. There was also a trend towards increased intratumoural CD8+ T cells and HLA-G expression on tumour cells in HPV+ samples. qRT-PCR data demonstrated a general pattern of increased immune activation and suppression mechanisms in HPV+ samples. Additionally, a combined score of intratumoural and invasive margin FoxP3 infiltration was significantly associated with disease-specific survival (P < 0.05).
Conclusions: These data demonstrate significant differences in the immune cell profile of HPV+ and HPV- HNSCC. This study identifies several possible targets for immunotherapy and possible prognostic markers (FoxP3 and HLA-G) that may be specific to HNSCC.
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010 Sep-Oct;60(5):277–300. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous