

Extracorporeal life support for acute respiratory failure. A systematic review and metaanalysis
- PMID: 24724902
- PMCID: PMC5467087
- DOI: 10.1513/AnnalsATS.201401-012OC
Extracorporeal life support for acute respiratory failure. A systematic review and metaanalysis
Abstract
Rationale: Extracorporeal life support (ECLS) for acute respiratory failure has increased as a result of technological advancements and promising results from recent studies as compared with historical trials.
Objectives: Systematically review the effect of ECLS compared with mechanical ventilation on mortality, length of stay, and adverse events in respiratory failure.
Methods: Data sources included were MEDLINE, EMBASE, and CENTRAL (through to October 2013). Any randomized controlled trial (RCT) or observational study comparing ECLS to mechanical ventilation in adults was used. Two authors independently abstracted the data. Our primary outcome was mortality. Secondary outcomes included intensive care unit length of stay, hospital length of stay, and adverse events. A sensitivity analysis was performed restricted to RCTs and quasi-RCTs, and a number of predefined subgroups were identified to explore heterogeneity.
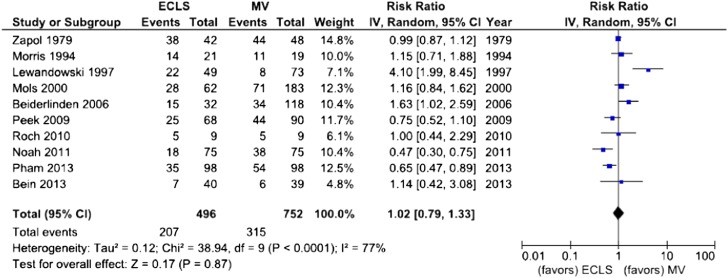
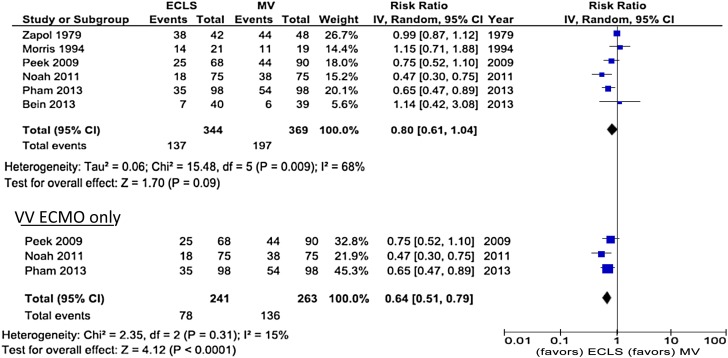
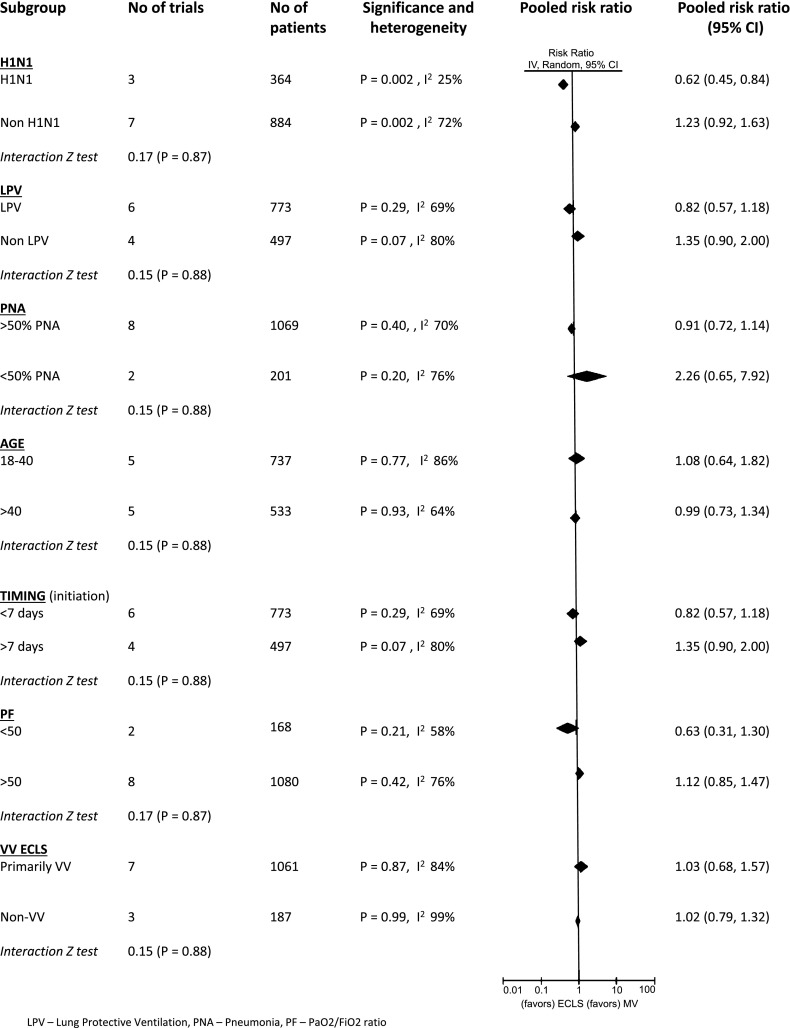
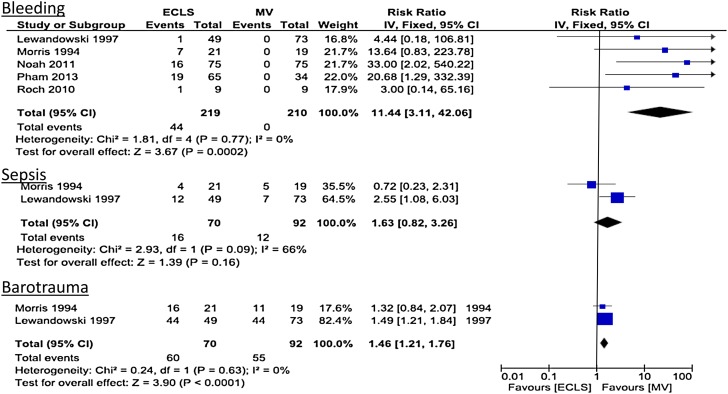
Measurements and main results: Ten studies (four RCTs, six observational studies, 1,248 patients) were included. There was no significant difference in hospital mortality with ECLS as compared with mechanical ventilation (risk ratio [RR], 1.02; 95% confidence interval [CI], 0.79-1.33; I(2) = 77%). When restricted to venovenous ECLS studies of randomized trials and quasi-randomized trials (three studies; 504 patients), there was a decrease in mortality with ECLS compared with mechanical ventilation (RR, 0.64; 95% CI, 0.51-0.79; I(2) = 15%). There were insufficient study-level data to evaluate most secondary outcomes. Bleeding was significantly greater in the ECLS group (RR, 11.44; 95% CI, 3.11-42.06; I(2) = 0%). In the H1N1 subgroup (three studies; 364 patients), ECLS was associated with significantly lower hospital mortality (RR, 0.62; 95% CI, 0.45-0.8; I(2) = 25%).
Conclusions: ECLS was not associated with a mortality benefit in patients with acute respiratory failure. However, a significant mortality benefit was seen when restricted to higher-quality studies of venovenous ECLS. Patients with H1N1-acute respiratory distress syndrome represent a subgroup that may benefit from ECLS. Future studies are needed to confirm the efficacy of ECLS as well as the optimal configuration, indications, and timing for adult patients with respiratory failure.
Keywords: adult; critical care; extracorporeal life support; intensive care units; respiratory distress syndrome; systematic review.
Figures
Comment in
-
Extracorporeal life support. A "breath-taking" technology?Ann Am Thorac Soc. 2014 Jun;11(5):799-801. doi: 10.1513/AnnalsATS.201403-136ED. Ann Am Thorac Soc. 2014. PMID: 24936694 No abstract available.
-
Extracorporeal life support.Ann Am Thorac Soc. 2014 Jul;11(6):992. doi: 10.1513/AnnalsATS.201404-182LE. Ann Am Thorac Soc. 2014. PMID: 25032875 No abstract available.
-
Reply: extracorporeal life support.Ann Am Thorac Soc. 2014 Jul;11(6):993. doi: 10.1513/AnnalsATS.201405-195LE. Ann Am Thorac Soc. 2014. PMID: 25032876 Free PMC article. No abstract available.
References
-
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307:2526–2533. - PubMed
-
- The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–1308. - PubMed
-
- Papazian L, Forel JM, Gacouin A, Penot-Ragon C, Perrin G, Loundou A, Jaber S, Arnal JM, Perez D, Seghboyan JM, et al. Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med. 2010;363:1107–1116. - PubMed
-
- Fan E, Wilcox ME, Brower RG, Stewart TE, Mehta S, Lapinsky SE, Meade MO, Ferguson ND. Recruitment maneuvers for acute lung injury: a systematic review. Am J Respir Crit Care Med. 2008;178:1156–1163. - PubMed
-
- Sud S, Sud M, Friedrich JO, Meade MO, Ferguson ND, Wunsch H, Adhikari NK. High frequency oscillation in patients with acute lung injury and acute respiratory distress syndrome (ARDS): systematic review and meta-analysis. BMJ. 2010;340:c2327. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
