

Screening and detection advances in magnetic resonance image-guided prostate biopsy
- PMID: 24725492
- PMCID: PMC3986723
- DOI: 10.1016/j.ucl.2014.01.007
Screening and detection advances in magnetic resonance image-guided prostate biopsy
Abstract
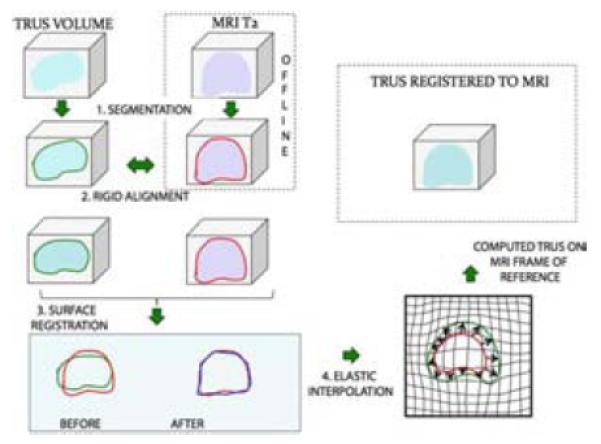
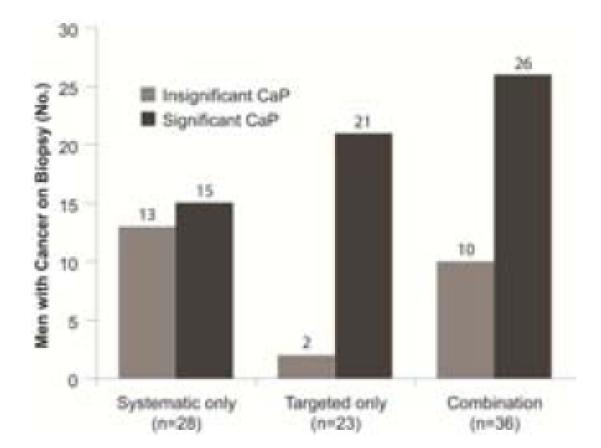
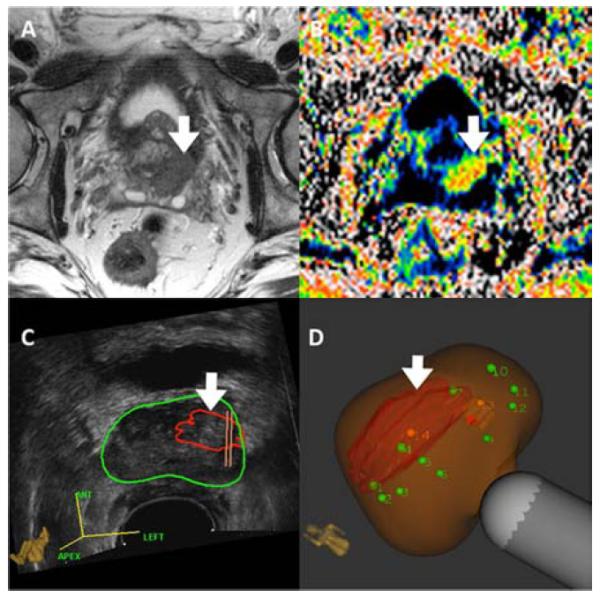
Multiparametric magnetic resonance imaging (MRI) has provided a method for visualizing prostate cancer. MRI-ultrasonography fusion allows prostate biopsy to be performed quickly, on an outpatient basis, using the transrectal technique. Targeted biopsies are more sensitive for detection of prostate cancer than nontargeted, systematic biopsies and detect more significant prostate cancers and fewer insignificant cancers than conventional biopsies. A negative MRI scan should not defer biopsy. Two groups who will especially benefit from targeted prostate biopsy are men with low-risk lesions in active surveillance and men with increased prostate-specific antigen levels and previous negative conventional biopsies.
Keywords: Fusion biopsy; Magnetic resonance imaging; Prostate cancer; Prostate-specific antigen; Targeted prostate biopsy; Transrectal ultrasonography; Ultrasonography.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures





References
-
- Silletti JP, Gordon GJ, Bueno R, Jaklitsch M, Loughlin KR. Prostate biopsy: past, present, and future. Urology. 2007 Mar;69(3):413–416. - PubMed
-
- Hodge KK, McNeal JE, Terris MK, Stamey TA. Random systematic versus directed ultrasound guided transrectal core biopsies of the prostate. The Journal of urology. 1989 Jul;142(1):71–74. discussion 74-75. - PubMed
-
- King CR, McNeal JE, Gill H, Presti JC., Jr. Extended prostate biopsy scheme improves reliability of Gleason grading: implications for radiotherapy patients. Int J Radiat Oncol Biol Phys. 2004 Jun 1;59(2):386–391. - PubMed
-
- Hricak H, Williams RD, Spring DB, et al. Anatomy and pathology of the male pelvis by magnetic resonance imaging. AJR. American journal of roentgenology. 1983 Dec;141(6):1101–1110. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
