

Complete clinical regression of a BRAF V600E-mutant pediatric glioblastoma multiforme after BRAF inhibitor therapy
- PMID: 24725538
- PMCID: PMC3996187
- DOI: 10.1186/1471-2407-14-258
Complete clinical regression of a BRAF V600E-mutant pediatric glioblastoma multiforme after BRAF inhibitor therapy
Abstract
Background: Standard therapies for high grade glioma have failed to substantially improve survival and are associated with significant morbidity. At relapse, high grade gliomas, such as glioblastoma multiforme, are refractory to therapy and universally fatal. BRAF V600E-mutations have been described in a modest 6% to 7% of primary central nervous system (CNS) tumors, but with increased prevalence in the pediatric population and in certain brain tumor subtypes. The use of BRAF inhibitors have transformed melanoma therapy however their use in brain tumors remains unproven.
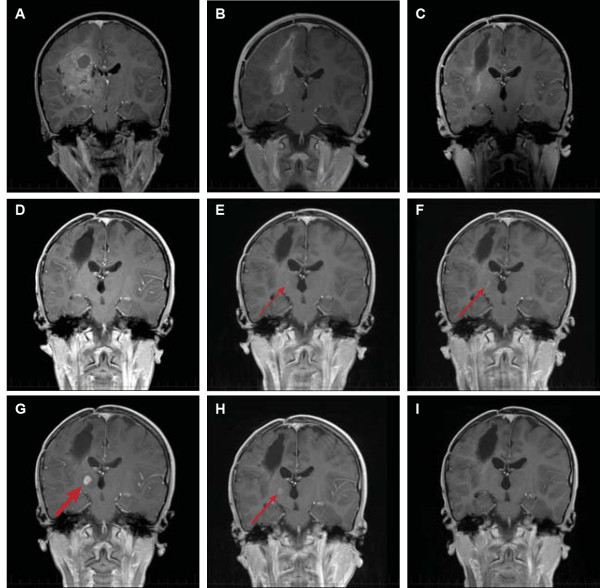
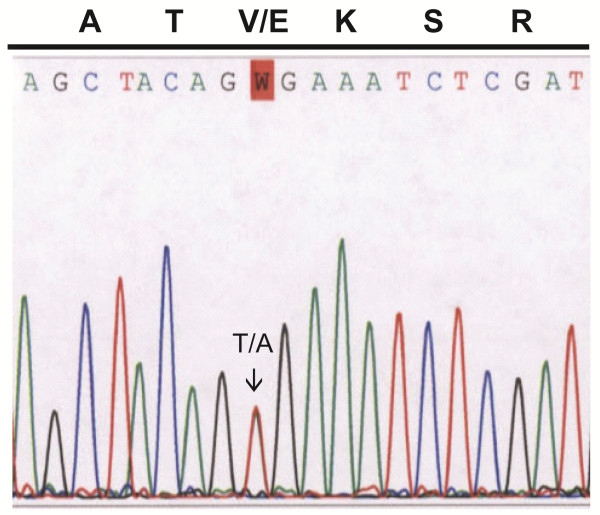
Case presentation: We describe the pediatric case of a now 12 year old Caucasian male who originally presented at age 9 with a right fronto-parietal glioblastoma multiforme that recurred 2 ½ years from diagnosis. Molecular analysis of the primary tumor revealed a BRAF V600E mutation and the patient was placed on the BRAF inhibitor vemurafenib. A complete response was observed after 4 months of therapy and remains sustained at 6 months.
Conclusion: This is the first report of a complete response of relapsed glioblastoma multiforme to targeted BRAF inhibitor therapy. While not a predominant mutation in glioblastoma multiforme, the increased prevalence of BRAF V600 mutations in pediatric CNS tumors and certain subtypes marks a population to whom this therapy could be applied. Response to this therapy suggests that BRAF inhibitors can affect primary CNS lesions when a documented and targetable mutation is present.
Figures
References
-
- Schindler G, Capper D, Meyer J, Janzarik W, Omran H, Herold-Mende C, Schmieder K, Wesseling P, Mawrin C, Hasselblatt M, Louis DN, Korshunov A, Pfister S, Hartmann C, Paulus W, Reifenberger G, von Deimling A. Analysis of BRAF V600E mutation in 1,320 nervous system tumors reveals high mutation frequencies in pleomorphic xanthoastrocytoma, ganglioglioma and extra-cerebellar pilocytic astrocytoma. Acta Neuropathol. 2011;121:397–405. doi: 10.1007/s00401-011-0802-6. - DOI - PubMed
-
- Schiffman JD, Hodgson JG, VandenBerg SR, Flaherty P, Polley MY, Yu M, Fisher PG, Rowitch DH, Ford JM, Berger MS, Ji H, Gutmann DH, James CD. Oncogenic BRAF mutation with CDKN2A inactivation is characteristic of a subset of pediatric malignant astrocytomas. Cancer Res. 2010;70:512–519. doi: 10.1158/0008-5472.CAN-09-1851. - DOI - PMC - PubMed
-
- Flaherty KT, Robert C, Hersey P, Nathan P, Garbe C, Milhem M, Demidov LV, Hassel JC, Rutkowski P, Mohr P, Dummer R, Trefzer U, Larkin JM, Utikal J, Dreno B, Nyakas M, Middleton MR, Becker JC, Casey M, Sherman LJ, Wu FS, Ouellet D, Martin AM, Patel K, Schadendor F. Improved survival with MEK inhibition in BRAF-mutated melanoma. N Engl J Med. 2012;367:107–114. doi: 10.1056/NEJMoa1203421. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
