

Physiology and pathophysiology of iron in hemoglobin-associated diseases
- PMID: 24726864
- PMCID: PMC4940047
- DOI: 10.1016/j.freeradbiomed.2014.03.039
Physiology and pathophysiology of iron in hemoglobin-associated diseases
Abstract
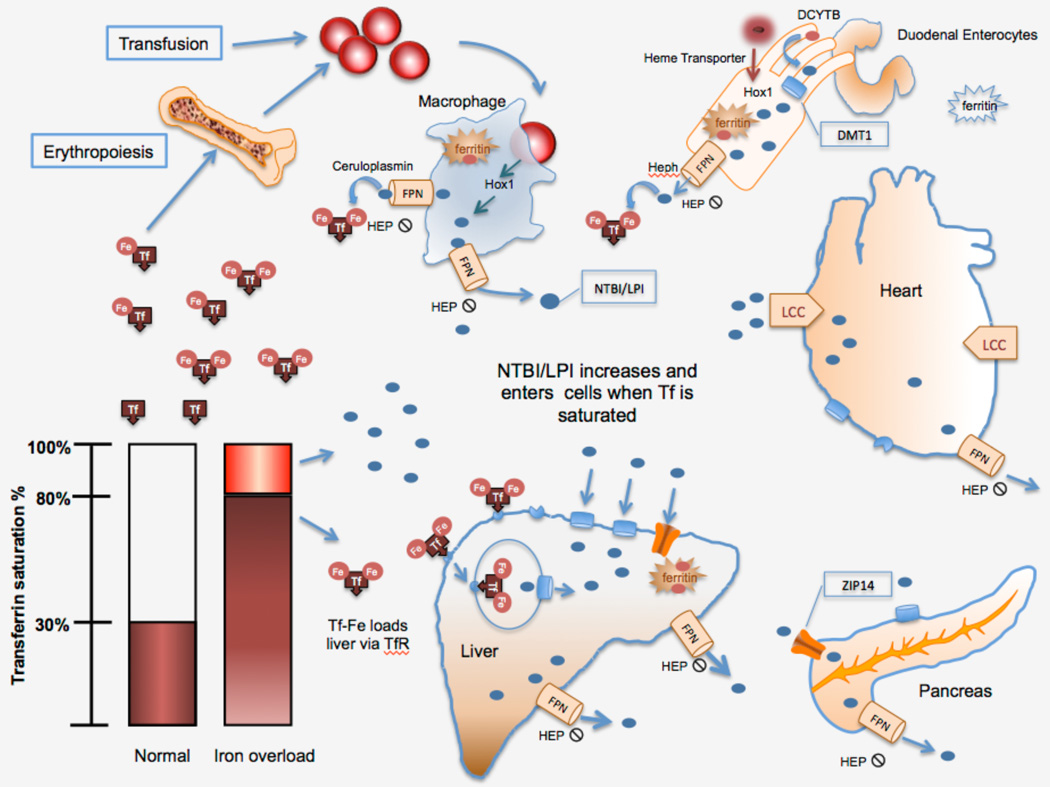
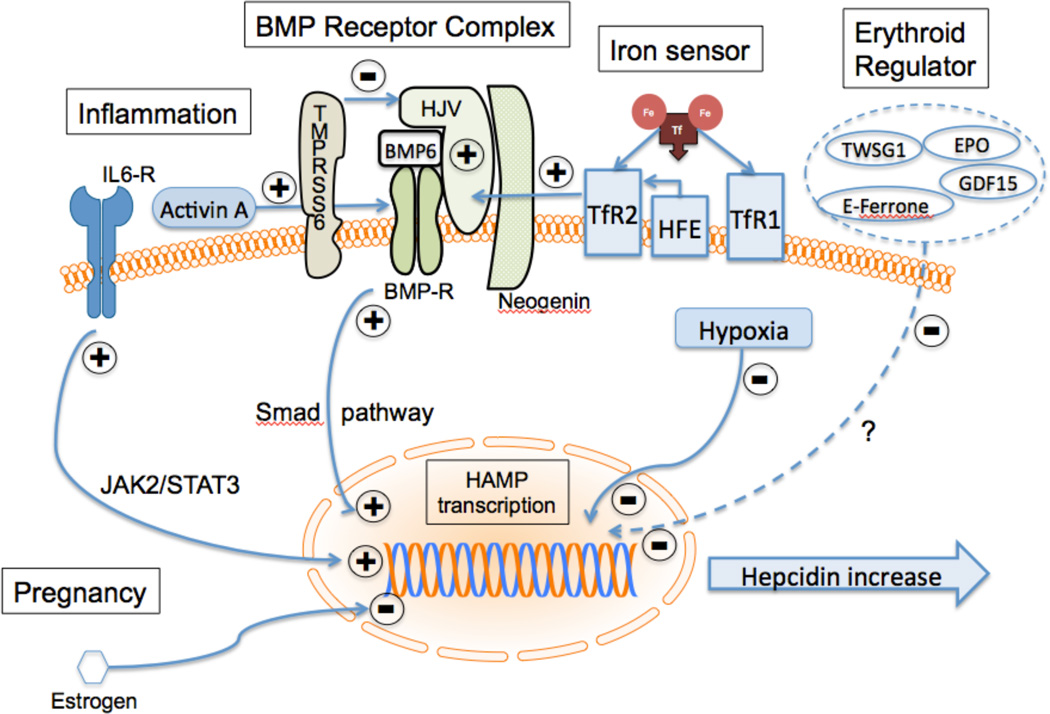
Iron overload and iron toxicity, whether because of increased absorption or iron loading from repeated transfusions, can be major causes of morbidity and mortality in a number of chronic anemias. Significant advances have been made in our understanding of iron homeostasis over the past decade. At the same time, advances in magnetic resonance imaging have allowed clinicians to monitor and quantify iron concentrations noninvasively in specific organs. Furthermore, effective iron chelators are now available, including preparations that can be taken orally. This has resulted in substantial improvement in mortality and morbidity for patients with severe chronic iron overload. This paper reviews the key points of iron homeostasis and attempts to place clinical observations in patients with transfusional iron overload in context with the current understanding of iron homeostasis in humans.
Keywords: Chelation; Hemochromatosis; Hemoglobinopathy; Iron overload; Iron toxicity; Magnetic resonance imaging; ROS; Sickle cell disease; Thalassemia; Transfusion.
Copyright © 2014 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest: Dr Coates is on the Speaker’s Bureau or consults for Novartis Pharma, Shire Pharma, Apo Pharma, and Celeron.
Figures
References
-
- Green R, Charlton R, Seftel H, Bothwell T, Mayet F, Adams B, Finch C, Layrisse M. Body iron excretion in man: a collaborative study. Am J Med. 1968;45:336–353. - PubMed
-
- Ganz T. Systemic iron homeostasis. Physiol Rev. 2013;93:1721–1741. - PubMed
-
- Frazer DM, Anderson GJ. The regulation of iron transport. BioFactors. 2013 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
