

Associations between primary healthcare and unplanned medical admissions in Norway: a multilevel analysis of the entire elderly population
- PMID: 24727427
- PMCID: PMC3987736
- DOI: 10.1136/bmjopen-2013-004293
Associations between primary healthcare and unplanned medical admissions in Norway: a multilevel analysis of the entire elderly population
Abstract
Objective: To examine if individual risk of unplanned medical admissions (UMAs) was associated with municipality general practitioner (GP) or long-term care (LTC) volume among the entire Norwegian elderly population.
Design: Cross-sectional population-based study.
Setting: 428 of 430 Norwegian municipalities in 2009.
Participants: All Norwegians aged ≥65 years (n=721 915; 56% women-15% of the total population).
Main outcome measure: Individual risk of UMA.
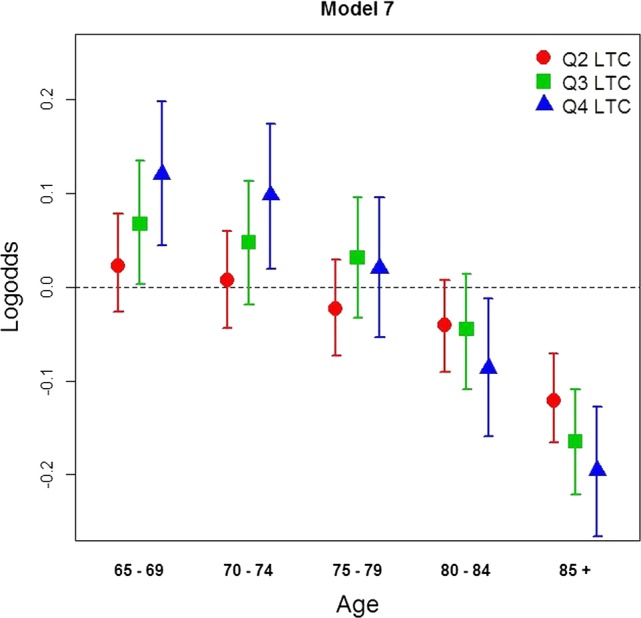
Results: Using a multilevel analytical framework, consisting of individuals (N=722 464) nested within municipalities (N=428), nested within local hospital areas (N=52) we found no association between municipality GP or LTC volume and UMAs. However, we found that higher LTC levels of provision were associated with fewer hospitalisations among the older age groups. A modest geographical variability was observed for UMA in adjusted analysis.
Conclusions: A higher primary healthcare volume was only associated with fewer UMAs among the oldest old in a universally accessible healthcare system.
Keywords: Long-term Care; Primary Care; Small Area Analyses; Unplanned Admissions.
Figures
Similar articles
-
Older high-cost patients in Norwegian somatic hospitals: a register-based study of patient characteristics.BMJ Open. 2023 Oct 4;13(10):e074411. doi: 10.1136/bmjopen-2023-074411. BMJ Open. 2023. PMID: 37793934 Free PMC article.
-
Does long-term care use within primary health care reduce hospital use among older people in Norway? A national five-year population-based observational study.BMC Health Serv Res. 2011 Oct 26;11:287. doi: 10.1186/1472-6963-11-287. BMC Health Serv Res. 2011. PMID: 22029775 Free PMC article.
-
Modelling resource requirements and physician staffing to provide virtual urgent medical care for residents of long-term care homes: a cross-sectional study.CMAJ Open. 2020 Aug 20;8(3):E514-E521. doi: 10.9778/cmajo.20200098. Print 2020 Jul-Sep. CMAJ Open. 2020. PMID: 32819964 Free PMC article.
-
Gender differences in health care use among the elderly population in areas of Norway and Finland. A cross-sectional analysis based on the HUNT study and the FINRISK Senior Survey.BMC Health Serv Res. 2006 Sep 4;6:110. doi: 10.1186/1472-6963-6-110. BMC Health Serv Res. 2006. PMID: 16952306 Free PMC article.
-
Regional variation in hospital care at the end-of-life of Dutch patients with lung cancer exists and is not correlated with primary and long-term care.Int J Qual Health Care. 2020 May 20;32(3):190-195. doi: 10.1093/intqhc/mzaa004. Int J Qual Health Care. 2020. PMID: 32186705 Free PMC article.
Cited by
-
Geographical Accessibility of Community Health Assist System General Practitioners for the Elderly Population in Singapore: A Case Study on the Elderly Living in Housing Development Board Flats.Int J Environ Res Public Health. 2018 Sep 12;15(9):1988. doi: 10.3390/ijerph15091988. Int J Environ Res Public Health. 2018. PMID: 30213094 Free PMC article.
-
Characteristics and predictors for hospitalizations of home-dwelling older persons receiving community care: a cohort study from Norway.BMC Geriatr. 2018 Sep 3;18(1):203. doi: 10.1186/s12877-018-0887-z. BMC Geriatr. 2018. PMID: 30176794 Free PMC article.
-
Contact with primary health care physicians before an acute hospitalisation.Scand J Prim Health Care. 2019 Sep;37(3):283-293. doi: 10.1080/02813432.2019.1639900. Epub 2019 Jul 9. Scand J Prim Health Care. 2019. PMID: 31286825 Free PMC article.
-
Older high-cost patients in Norwegian somatic hospitals: a register-based study of patient characteristics.BMJ Open. 2023 Oct 4;13(10):e074411. doi: 10.1136/bmjopen-2023-074411. BMJ Open. 2023. PMID: 37793934 Free PMC article.
-
Sociodemographic and health characteristics, rather than primary care supply, are major drivers of geographic variation in preventable hospitalizations in Australia.Med Care. 2015 May;53(5):436-45. doi: 10.1097/MLR.0000000000000342. Med Care. 2015. PMID: 25793270 Free PMC article.
References
-
- Blunt I, Bardsley M, Dixon J. Trends in emergency admissions in England 2004-2009. Nuffield Trust: Nuffield Trust, 2010
-
- Pitts SR, Pines JM, Handrigan MT, et al. National trends in emergency department occupancy, 2001 to 2008: effect of inpatient admissions versus emergency department practice intensity. Ann Emerg Med 2012;60:679–86 - PubMed
-
- Covinsky KE, Pierluissi E, Johnston CB. Hospitalization-associated disability: ‘She was probably able to ambulate, but I'm not sure’. JAMA 2011;306:1782–93 - PubMed
-
- Starfield B. Primary care: balancing health needs, services, and technology. 1st edn Oxford University Press, 1998
-
- Reid RJ, Coleman K, Johnson EA, et al. The group health medical home at year two: cost savings, higher patient satisfaction, and less burnout for providers. Health Aff 2010;29:835–43 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources