

Immunosuppression in acutely decompensated cirrhosis is mediated by prostaglandin E2
- PMID: 24728410
- PMCID: PMC5369639
- DOI: 10.1038/nm.3516
Immunosuppression in acutely decompensated cirrhosis is mediated by prostaglandin E2
Abstract
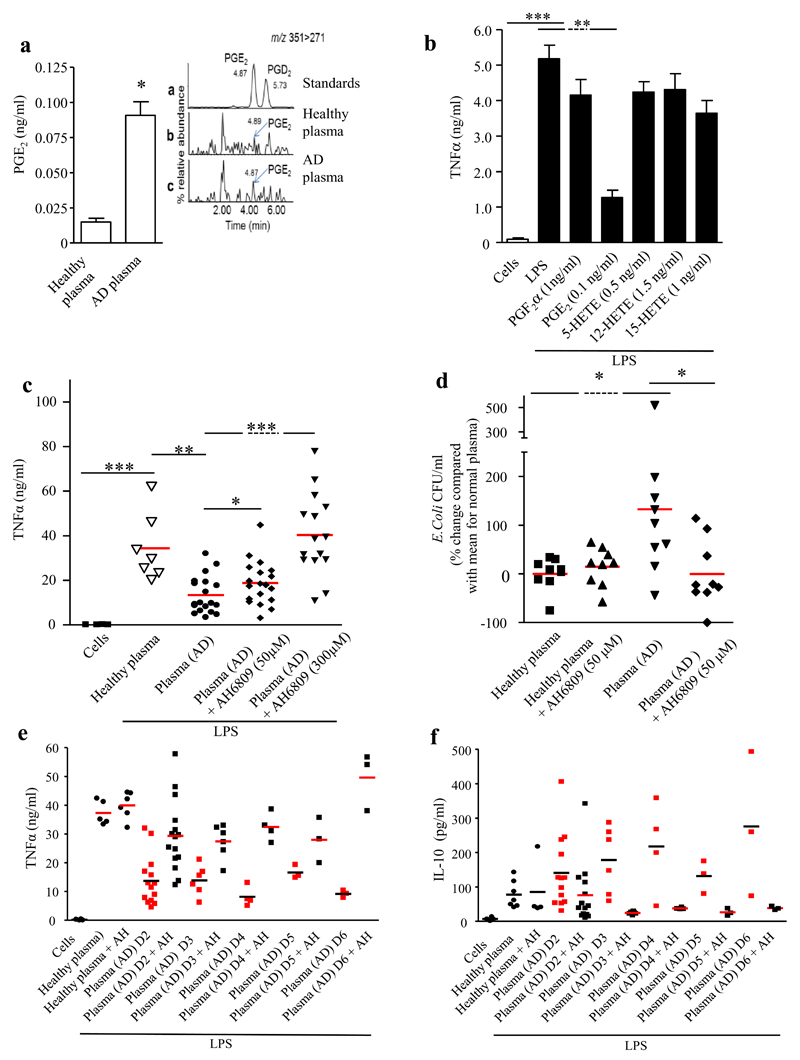
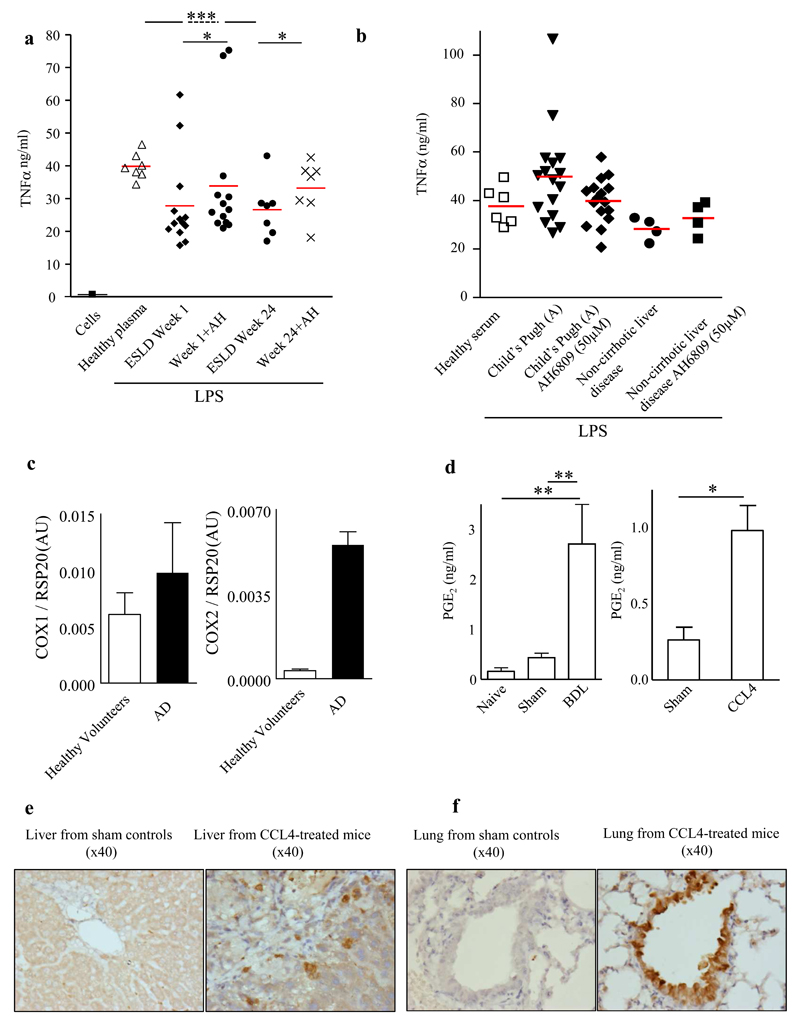
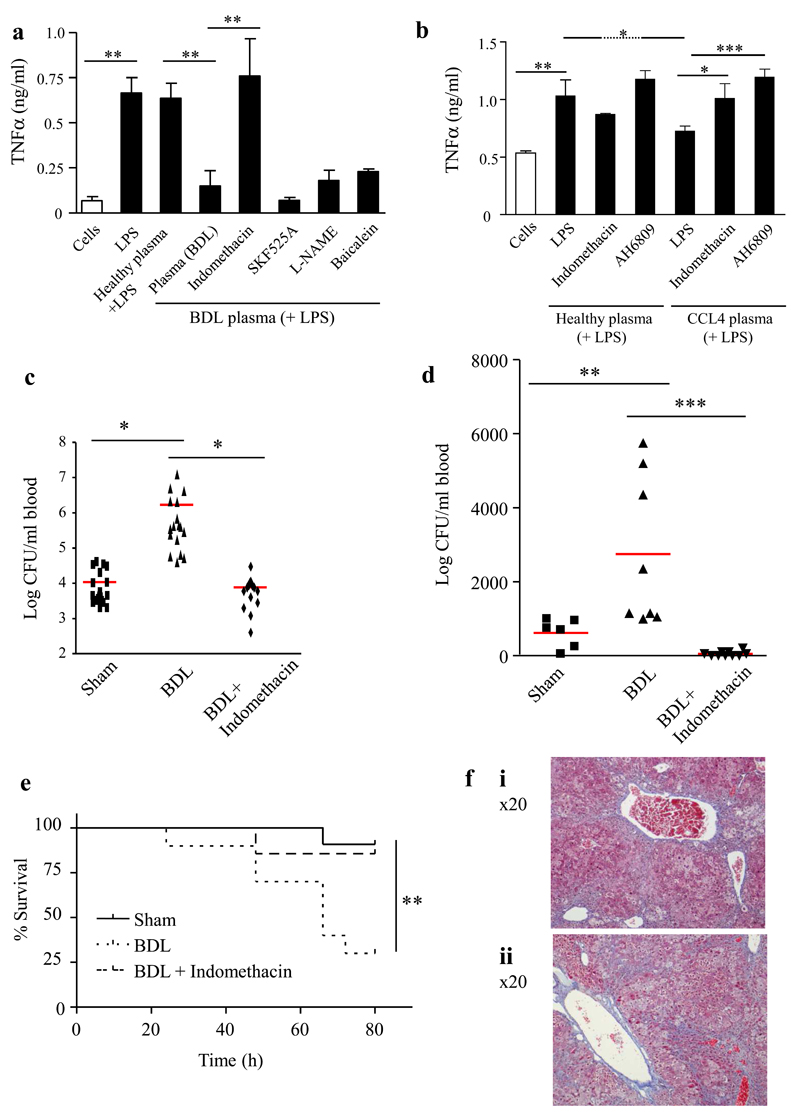
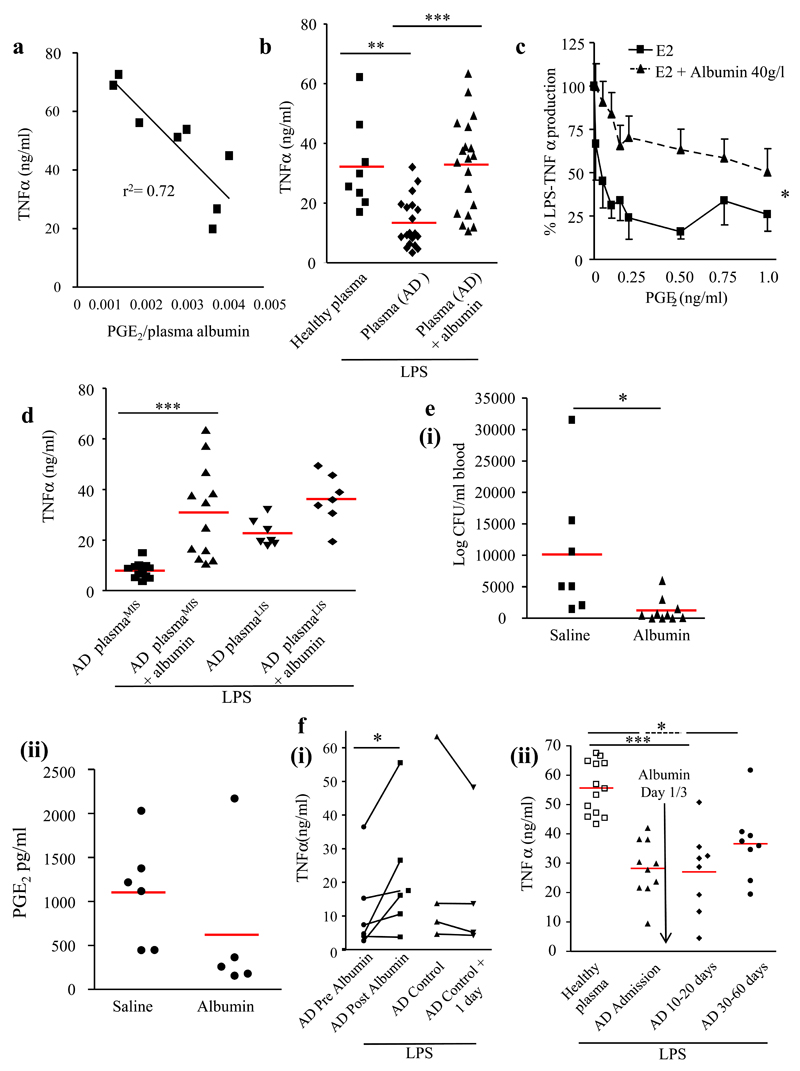
Liver disease is one of the leading causes of death worldwide. Patients with cirrhosis display an increased predisposition to and mortality from infection due to multimodal defects in the innate immune system; however, the causative mechanism has remained elusive. We present evidence that the cyclooxygenase (COX)-derived eicosanoid prostaglandin E2 (PGE2) drives cirrhosis-associated immunosuppression. We observed elevated circulating concentrations (more than seven times as high as in healthy volunteers) of PGE2 in patients with acute decompensation of cirrhosis. Plasma from these and patients with end-stage liver disease (ESLD) suppressed macrophage proinflammatory cytokine secretion and bacterial killing in vitro in a PGE2-dependent manner via the prostanoid type E receptor-2 (EP2), effects not seen with plasma from patients with stable cirrhosis (Child-Pugh score grade A). Albumin, which reduces PGE2 bioavailability, was decreased in the serum of patients with acute decompensation or ESLD (<30 mg/dl) and appears to have a role in modulating PGE2-mediated immune dysfunction. In vivo administration of human albumin solution to these patients significantly improved the plasma-induced impairment of macrophage proinflammatory cytokine production in vitro. Two mouse models of liver injury (bile duct ligation and carbon tetrachloride) also exhibited elevated PGE2, reduced circulating albumin concentrations and EP2-mediated immunosuppression. Treatment with COX inhibitors or albumin restored immune competence and survival following infection with group B Streptococcus. Taken together, human albumin solution infusions may be used to reduce circulating PGE2 levels, attenuating immune suppression and reducing the risk of infection in patients with acutely decompensated cirrhosis or ESLD.
Figures
Comment in
-
Innate immunity: A COX detox for the immune system?Nat Rev Immunol. 2014 Jun;14(6):358. doi: 10.1038/nri3686. Epub 2014 May 6. Nat Rev Immunol. 2014. PMID: 24798368 No abstract available.
-
Tying up PGE2 with albumin to relieve immunosuppression in cirrhosis.Nat Med. 2014 May;20(5):467-9. doi: 10.1038/nm.3553. Nat Med. 2014. PMID: 24804750 No abstract available.
-
Prostaglandin E2 -mediated immunosuppression and the role of albumin as its modulator.Hepatology. 2015 Mar;61(3):1080-2. doi: 10.1002/hep.27644. Epub 2015 Jan 28. Hepatology. 2015. PMID: 25482406 No abstract available.
References
-
- Lim YS, Kim WR. The global impact of hepatic fibrosis and end-stage liver disease. Clin Liver Dis. 2008;12:733–746. vii. - PubMed
-
- Fernandez J, et al. Bacterial infections in cirrhosis: epidemiological changes with invasive procedures and norfloxacin prophylaxis. Hepatology. 2002;35:140–148. - PubMed
-
- Navasa M, Fernandez J, Rodes J. Bacterial infections in liver cirrhosis. Italian journal of gastroenterology and hepatology. 1999;31:616–625. - PubMed
-
- O'Brien AJ, Welch CA, Singer M, Harrison DA. Prevalence and outcome of cirrhosis patients admitted to UK intensive care: a comparison against dialysis-dependent chronic renal failure patients. Intensive care medicine. 2012;38:991–1000. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
