

Xpert MTB/RIF assay shortens airborne isolation for hospitalized patients with presumptive tuberculosis in the United States
- PMID: 24729506
- PMCID: PMC4133562
- DOI: 10.1093/cid/ciu212
Xpert MTB/RIF assay shortens airborne isolation for hospitalized patients with presumptive tuberculosis in the United States
Abstract
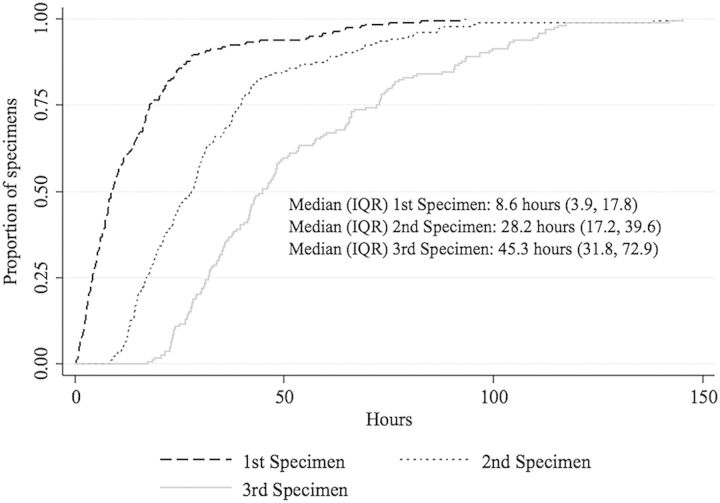
Background: In the United States, individuals with presumptive pulmonary tuberculosis are placed in airborne infection isolation (AII) and assessed by smear microscopy on 3 respiratory specimens collected 8-24 hours apart. Xpert MTB/RIF assay (Xpert) on 1, 2, or 3 specimens may be more efficient for determining AII discontinuation.
Methods: This single-center, observational cohort study of inpatients with presumptive pulmonary tuberculosis enrolled adults with 1 or more sputum specimens submitted for smear microscopy. Smear microscopy and Xpert were performed on each sputum specimen. Clinicians were blinded to Xpert results. The primary endpoint was AII duration. Secondary endpoints were laboratory processing time, strategy-based tuberculosis detection, and sensitivity and specificity.
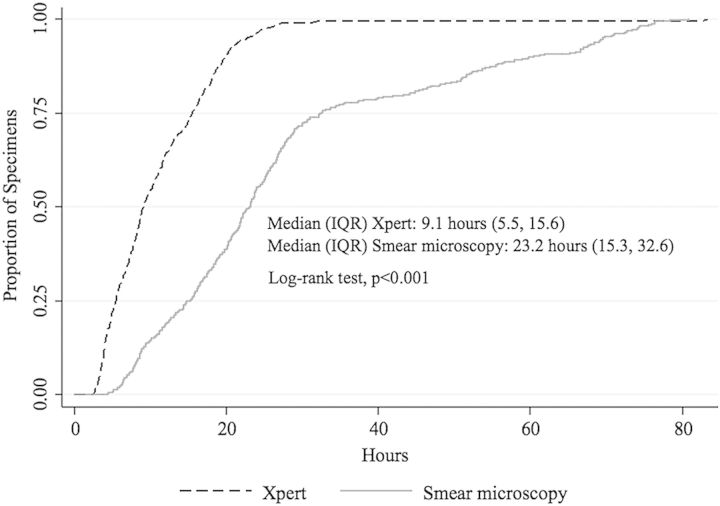
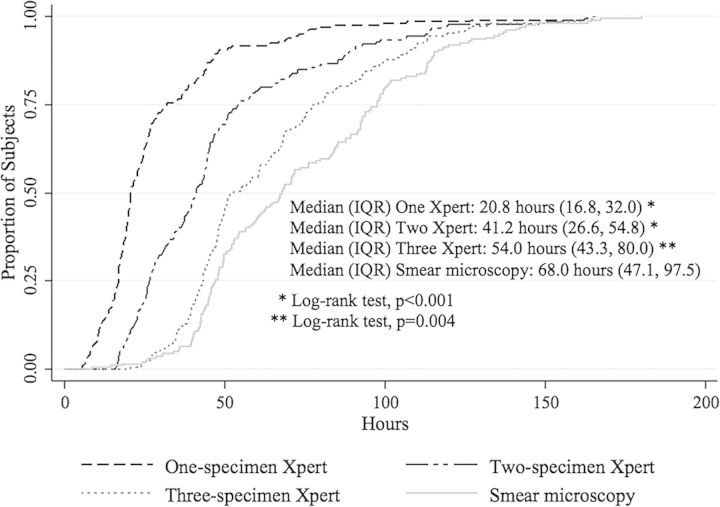
Results: Among 207 subjects, the median AII duration was 68.0 hours (interquartile range [IQR], 47.1-97.5) for smear microscopy compared with 20.8 hours (IQR, 16.8-32.0) for the 1-specimen Xpert, 41.2 hours (IQR, 26.6-54.8) for the 2-specimen Xpert, and 54.0 hours (IQR, 43.3-80.0) for the 3-specimen Xpert strategies (P ≤ .004). Median laboratory processing time for smear microscopy was 2.5 times as long as Xpert (P < .001). The 2- and 3-specimen Xpert and smear microscopy strategies captured all 6 tuberculosis cases. The 1-specimen Xpert strategy missed 1 case. No difference was observed between smear microscopy and Xpert in sensitivity or specificity for detection of Mycobacterium tuberculosis.
Conclusions: Xpert-based strategies significantly reduced AII duration compared with the smear-based strategy. The 2-specimen Xpert strategy was most efficient in minimizing AII time while identifying all tuberculosis cases among individuals with presumptive tuberculosis in this low-burden setting.
Keywords: United States; Xpert; infection control; tuberculosis.
© The Author 2014. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Dowdle WR. A strategic plan for the elimination of tuberculosis in the United States. MMWR Morb Mortal Wkly Rep. 1989;38(suppl 3):1–25. - PubMed
-
- Centers for Disease Control and Prevention. Atlanta, GA: US Department of Health and Human Services,; 2013. Reported tuberculosis in the United States, 2012.
-
- Jensen PA, Lambert LA, Iademarco MF, Ridzon R. Guidelines for preventing the transmission of Mycobacterium tuberculosis in health-care settings, 2005. MMWR Recomm Rep. 2005;54:1–141. - PubMed
-
- Steingart KR, Henry M, Ng V, et al. Fluorescence versus conventional sputum smear microscopy for tuberculosis: a systematic review. Lancet Infect Dis. 2006;6:570–81. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
